Deafness is a global public health problem. More than 1.5 billion people (nearly 20% of the global population) live with hearing loss, and 430 million of them have disabling hearing loss, including 34 million children. In sub-Saharan Africa, nearly eight million children under the age of 15 have hearing loss [1,2]. This article, led by Marie Josée Tanon-Anoh, looks at the successes that have been made in the CÔte d’Ivoire to care for deaf children.
Each year, 740,000 children (about six per 1000 live births) have hearing loss in the first month of life in middle- and low-income countries, compared to 28,000 (about two per 1,000 live births) in high-income countries [3]. In Côte d’Ivoire (RCI) the prevalence of neonatal deafness is three to six per 1000 births [4,5]. Thus, with about 700,000 live births in 2020 and 2022 in RCI, we could estimate a number of deaf newborns ranging from 2100 to 4000 per year.
Moreover, WHO estimates that global hearing aid production covers just 3% of the need in low- and middle-income countries [1]. According to the WHO World Hearing Report [2], only 10% of deaf people requiring hearing aids have access to them in Africa. This article highlights the problem of deafness in Africa, particularly the care of deaf children in a context of countries that are under-medicalised and have limited income, such as Côte d’Ivoire.
Diagnosis of deafness in children in Côte d’Ivoire
The diagnosis of deafness in young children remains difficult because of the lack of resources in both public and private hospitals. There is also a lack of specialised staff: for example, there were only five audiologists for a population of nearly 27.5 million residents in 2021 [1]. As a result, the diagnosis of congenital deafness happens late [6], which negatively impacts the possibilities of hearing rehabilitation.
Access to care remains limited due to the insufficient number of specialists: about 80 ENT specialists practising in Côte d’Ivoire in 2021 (a ratio of three ENT doctors per one million inhabitants), 86% of whom practice in the economic capital Abidjan. These disparities between low-income and high-income countries are flagged in the latest WHO World Hearing Report. Indeed, among low-income countries, about 78% have less than one otolaryngologist per million people; 93% have less than one audiologist per million people, and only 17% have one or more speech therapists per million people [2].
"There were only five audiologists for a population of nearly 27.5 million residents in 2021"
According to hospital studies carried out in Côte d’Ivoire, sensorineural hearing loss is predominant: two out of three (60 -75%) cases of deafness in children are sensorineural [7,8]. The main aetiologies of these cases are summarised in Table I.
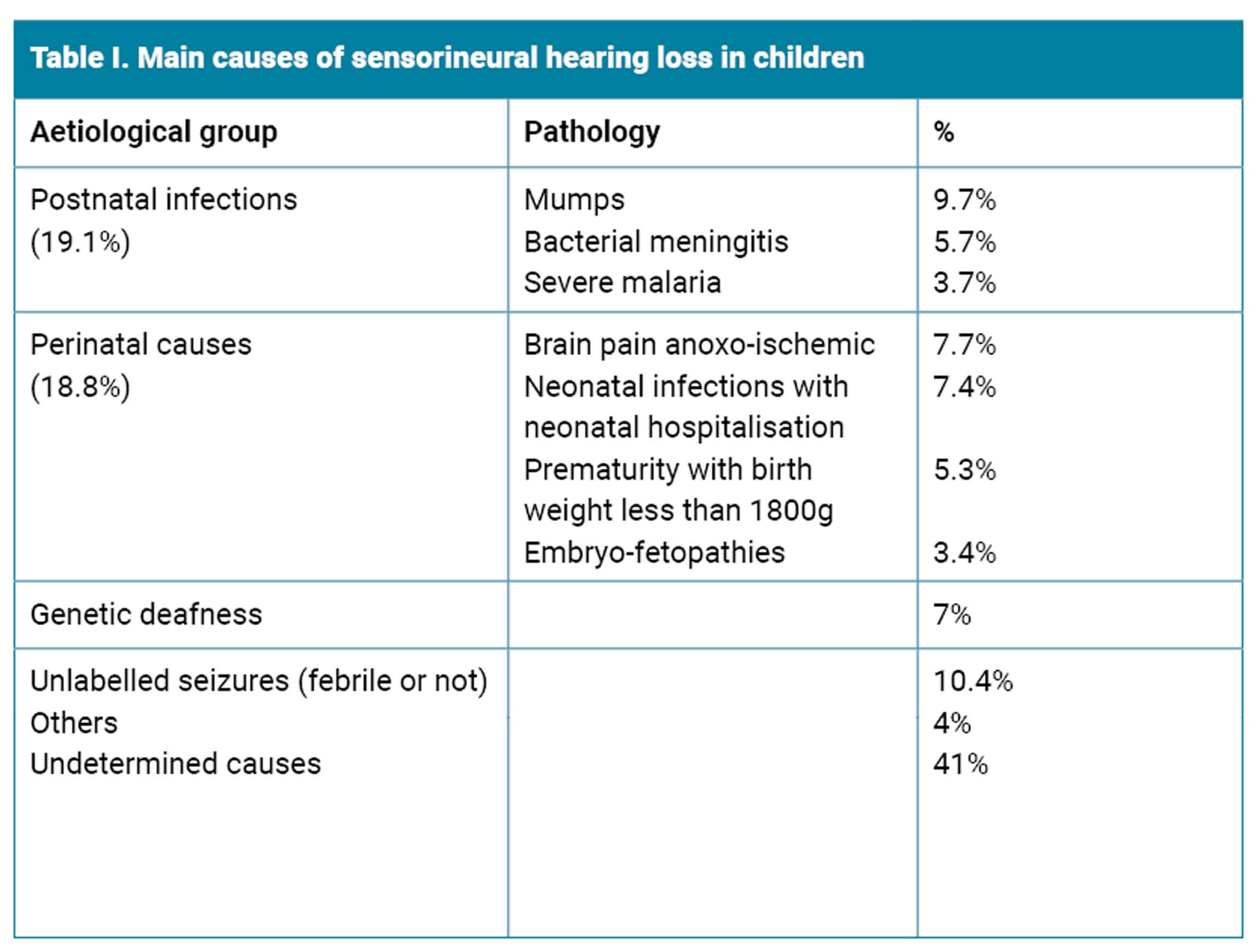
A severe to profound sensorineural hearing loss is found in more than half of the cases (45-64%) [7], for which the only method of hearing rehabilitation remains the cochlear implantation.Organisation of cochlear implantation in Côte d’Ivoire The care of congenital profoundly deaf children is still very difficult in Côte d’Ivoire, despite the recent introduction of cochlear implantation in December 2015. As of May 2023, 91 patients have been implanted in Abidjan (Figure 1), 95.5% of whom are children.
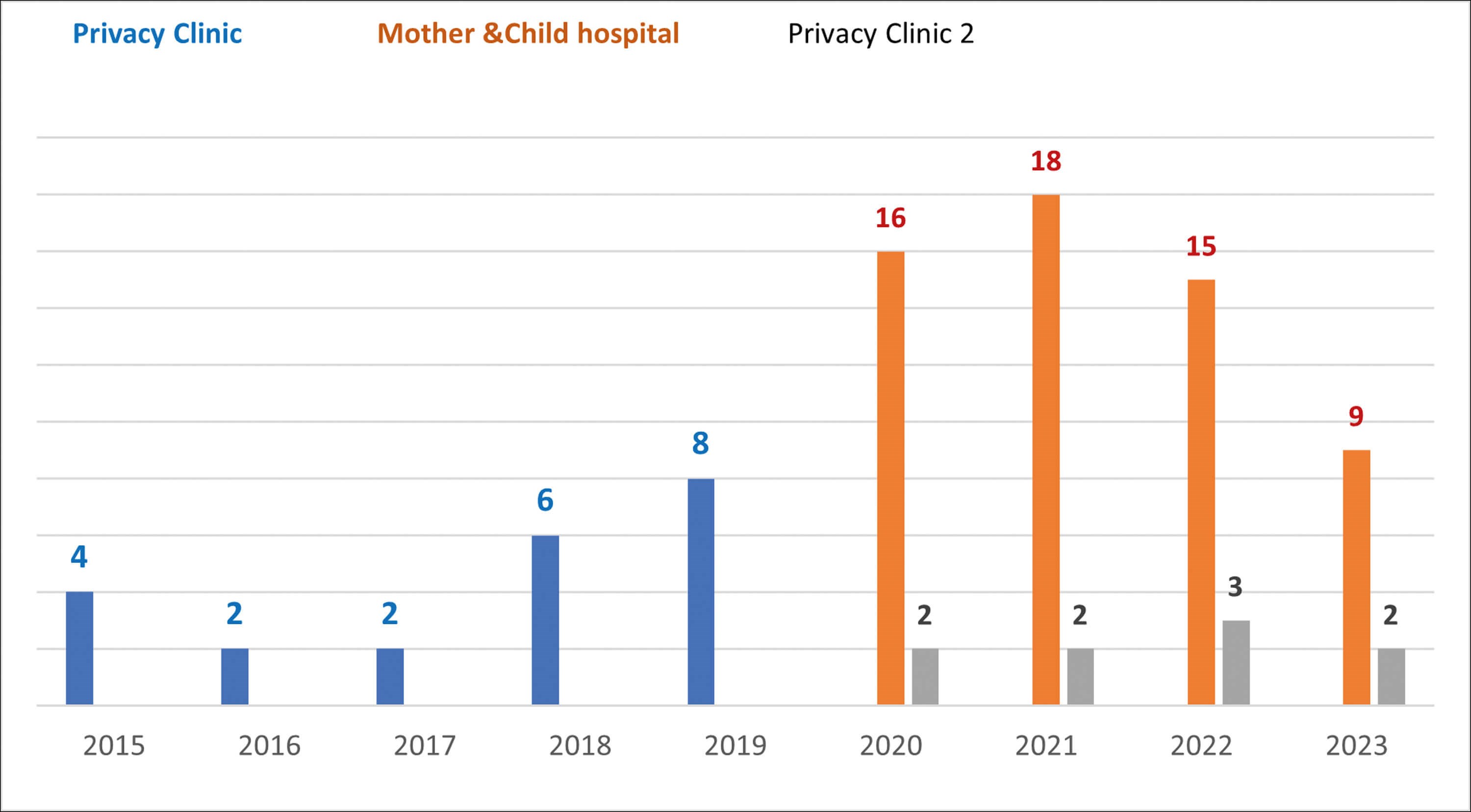
Figure 1. Distribution of patients by year and type of structure (from December 2015 to April 2023).
The average age of implanted children was 41 months (range: 25 months - 14 years 3 months). These were mainly cases of pre-lingual deafness (84/87 children). Some children had syndromic deafness, including Waardenburg syndrome (Figure 2).


Figure 2. Waardenburg syndrome and cochlear implant.
Given the proportion of severe to profound deafness in children, it can be concluded that cochlear implantation is insufficiently implemented in our country. There are many reasons for this. The lack of specialised staff is a major obstacle to opening more cochlear implantation centres in the territory. Indeed, the multidisciplinary team, including ENT surgeons, changes by audiologists, audioprosthetists, speech therapists and psychologists is the central link in any implantation procedure. With a ratio of less than one speech therapist per one million inhabitants in Côte d’Ivoire, speech therapy is a problem in our context (regularity, number of sessions per week). Prior to 2020, a centre had been organised solely for implantation surgery sessions in a private medical clinic. Since then, the opening of the Mother Child Hospital in Bingerville has provided comprehensive multidisciplinary care for deaf children (pre-implantation assessment and follow-up).
"As of May 2023, 91 patients have been implanted in Abidjan, 95.5% of whom are children"
The cost of cochlear implantation is also an essential limitation in our context [9]. The overall cost of rehabilitation, including pre-implantation imaging assessment, cochlear implant, surgery and postoperative hospitalisation, and speech therapy depends on the type of structure (hospital/private clinic). The funding sources of the procedures vary (Figure 3).
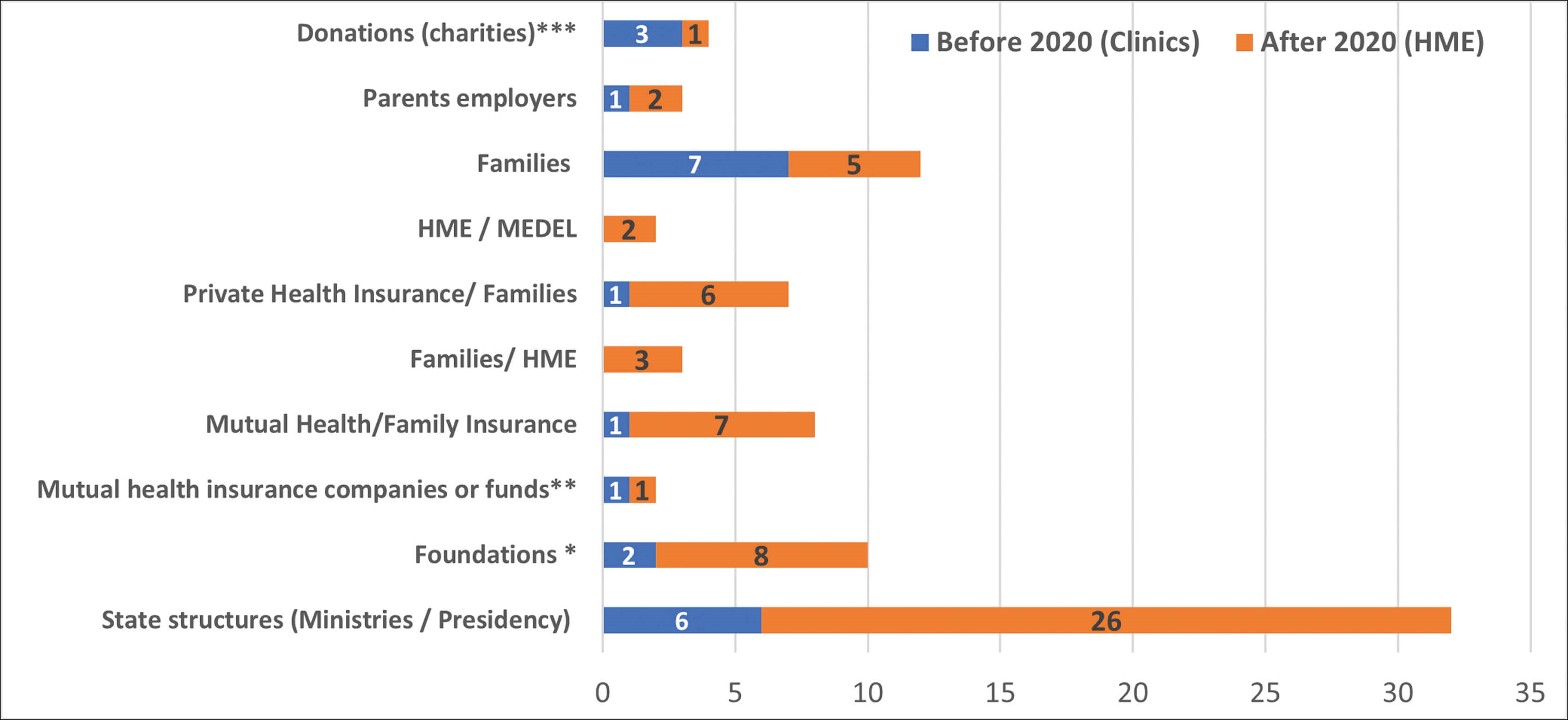
*** Donations: Association of ambassadors’ wives, NGO Padre Pio
** Military Contingency Fund
* Foundations (Magic system; Children of Africa)
Figure 3. Sources of funding for the cochlear implant procedure.
Universal health coverage has recently been implemented in Côte d’Ivoire and cochlear implants are not covered. However, a greater involvement of the state of Côte d’Ivoire through state structures has been noted since 2020.
The funding obtained does not cover accessories, which remain the responsibility of the families, outside the manufacturers’ guarantees, nor speech therapy sessions after the first year post implantation, which is a source of demotivation and irregularity in rehabilitation.
"This auditory rehabilitation has enabled the schooling of approximately 81-90% of children of school age, the majority of whom are in ordinary classes"
Despite these limitations, the first functional results of cochlear implantation in Côte d’Ivoire are promising because they come close to literature in terms of hearing gains and speech therapy results. This auditory rehabilitation has enabled the schooling of approximately 81-90% of children of school age, the majority of whom are in ordinary classes [6].
At the global level, there are advances in the management of childhood deafness, including early detection and diagnosis programmes, technological innovations and especially the organisation of cochlear implantation procedures, allowing wider access to hearing rehabilitation for deaf children.
In Africa and Côte d’Ivoire in particular, difficulties in the management of deafness persist. Outside the socio-cultural environment (beliefs, perception of deafness), the limitations related to insufficient equipment, qualified personnel, financial means that access to hearing rehabilitation methods for deaf children is very limited, with few specific social and educational facilities.
References
1. World Health Organization. Deafness and hearing loss. 2021.
www.who.int/health-topics/
hearing-loss
2. World Health Organization. World Report on Hearing. 2021.
www.who.int/multi-media/details/
world-report-on-hearing
3. Olusanya BO. Neonatal hearing screening and intervention in resource limited settings: an overview. Arch Dis Child 2012;97(7):654–9.
4. Tanon-Anoh MJ, Sanogo D, Kouassi KB. Newborn hearing screening in a developing country: results of a pilot study in Abidjan, Côte d’Ivoire. Int J Pediatr Otorhinolaryngol 2010;74(2):188–91.
5. Olusanya BO. Screening for neonatal deafness in resource-poor countries: challenges and solutions. Res Rep Neonatol 2015;5:51–64.
6. Tanon-Anoh MJ, Mafouo FS, Tea ZB, et al. Résultats des premières implantations cochléaires pédiatriques en Côte d’Ivoire. La Revue Africaine d’ORL et de Chirurgie Cervico-Faciale 2021;21(3):30–6.
7. Nogbou AHB épouse EHILE. Prise en charge des surdités de l’enfant au CHU de Cocody. [Thèse Med]. UFR des sciences médicales d’Abidjan. 2020.
8. Kein DJN. Morbidité́ hospitalière en ORL pédiatrique à l’hôpital mère enfant de Bingerville [Thèse Med]. UFR des sciences médicales d’Abidjan. 2021.
9. Tanon-Anoh MJ, Gbané M, Badou-Nguessan E, et al. Profil socio-épidémiologique des candidats à l’implantation cochléaire à Abidjan. La Revue Africaine d’ORL et de Chirurgie Cervico-Faciale 2021;21(2):41–8.
[All links last accessed November 2023]



