Sometimes patients with dizziness turn out to have slightly more unusual causes of their problem. Thomas Milner and Georgios Kontorinis describe their technique for managing patients who have a diagnosis of superior canal dehiscence as an identified cause of their dizziness.
Superior semicircular canal dehiscence (SSCD) is a defect in the integrity of the bony labyrinth of the superior semicircular canal resulting in a third window effect. SSCD was first described by Minor et al, who presented a case series of patients with noise or pressure-induced vertigo, associated with a computed tomography (CT) scan demonstrating bony dehiscence overlying the superior semicircular canal [1].
Patients typically present with vertigo induced by loud noises, or manoeuvres that alter middle ear pressure (e.g. sneezing). Occasionally a more chronic vertigo or disequilibrium can develop. During otological examination vertical torsional nystagmus can be elicited by applying tragal pressure (Hennebert’s sign) or exposure to loud noises (Tullio phenomenon). Audiological manifestations include low frequency conductive hearing loss, autophony and hypersensitivity to bone conducted sounds (e.g. eye movements). Pure tone audiograms reflect these findings with a low-frequency conductive hearing loss, associated with increased bone conduction.
High-resolution CT imaging of the temporal bones and vestibular evoked myogenic potentials (VEMPs) can be used to corroborate clinical findings. On fine-cut (0.5mm collimation or less) CT imaging reformatted to include cuts in the plane of and perpendicular to the superior semicircular canals, identification of bony dehiscence over the superior semicircular canal indicates SSCD [2] (see Figure 1). A full vestibular assessment is usually utilised in all patients suspected of having SSCD; however, VEMPs are the most useful vestibular diagnostic test. Both cervical and ocular VEMP thresholds are significantly lower in patients with SSCD, aiding diagnosis [3,4].
Following a diagnosis of SSCD, patients can opt for conservative management, or for surgical repair if symptoms are sufficiently disabling. Surgical correction of SSCD can either be performed via a middle fossa craniotomy (resurface) or via a transmastoid approach (obliteration); combined approaches have also been described, depending on the anatomic variations of every case.
This article describes the approach for performing transmastoid superior semicircular canal obliteration as well as a brief preoperative work out of such patients.
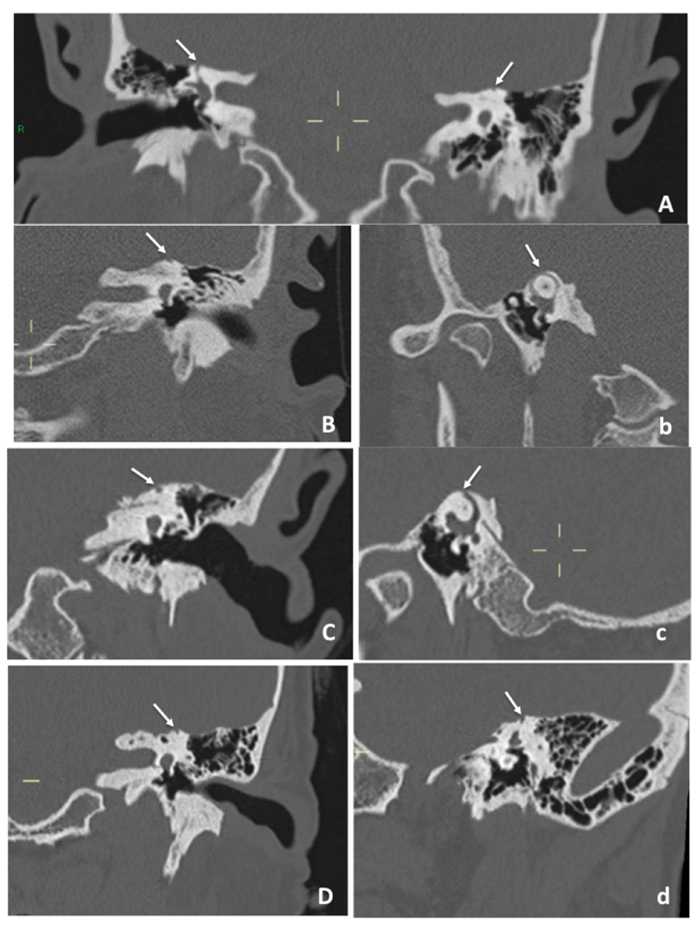
Figure 1. CT scans of a few of the patients with SSCD showing coronal (A, B, C and D) and sagittal and parasagittal oblique (b, c and d) sections of the temporal bone. The dehiscence is marked with white arrows and its extent can vary; in A the defect is bilateral.
Transmastoid obliteration
Preoperative approach
Among the most important aspects of managing the patients with SSCD are the utilisation of meticulous diagnostic batteries, sufficient trial of vestibular rehabilitation and very careful consultation. In our unit, the detailed history and clinical examination, which will raise the strong suspicion of SSCD, will be followed by high resolution CT of the temporal bones (Figure 1) as well as audiological and vestibular assessment including pure-tone audiometry (Figure 2C), tympanometry, cVEMPS (Figure 2A), dynamic posturography and lately six-canal video-Head-Impulse-Test (vHIT) (Figures 2B and b) and visual subjective vertical. Following the diagnosis of SSCD, the symptomatic patient will be referred for vestibular rehabilitation; should there be no improvement of the vestibular symptoms, the option of surgical intervention will be thoroughly explained, mainly to make the patient aware of the procedure, the related risks and benefits as well as the realistic expectations.
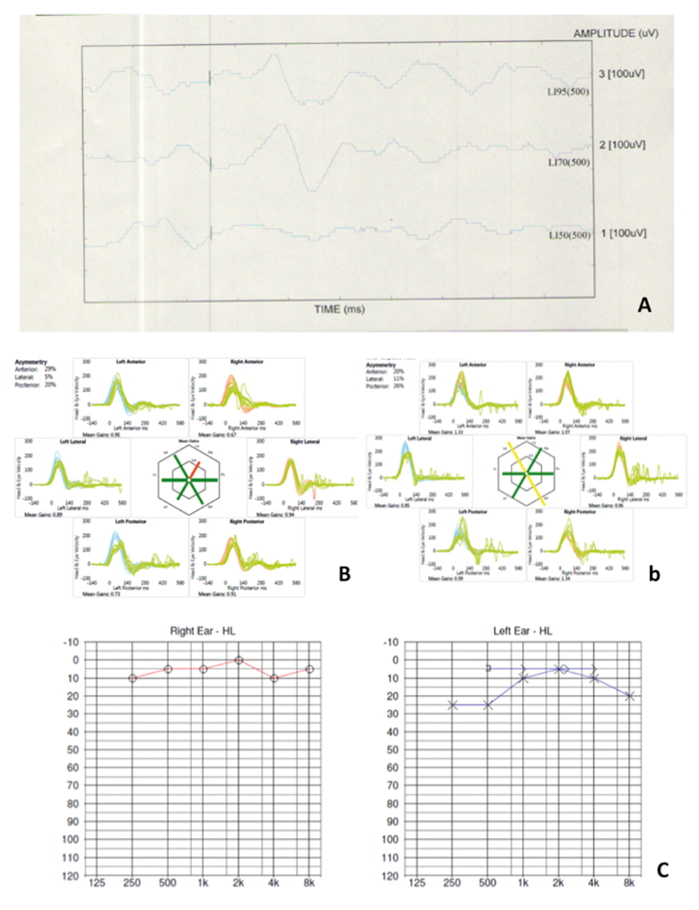
Figure 2. cVEMPS recorded at a level of 70dB (A), six-canal vHIT (B and b) and pure-tone audiogram showing low frequency air-bone gap (C) in patients with SSCD. Of note, the six-canal vHIT can show abnormal responses from not necessarily the superior semicircular canal. In the cases here we show reduced gain (B) in the right superior semicircular canal (patient with right SSCD) and increased gain in the left superior and right posterior semicircular canals (patient with left SSCD), possibly as result of the vestibular integration process.
Lately, we have implemented the use of three-dimensional prints of the patients’ skull that can demonstrate the bony defect (Figure 3). Such prints facilitate the surgical planning, improve the patients’ understanding of the condition as well as the planned procedure and, additionally, help with the juniors’ training.
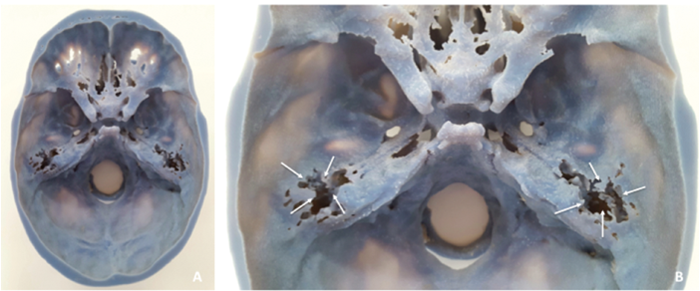
Figure 3. 3D-print of the skull of a patient with bilateral SSCD; of note the multiple tegmen bony defects (white arrows).
“Lately, we have implemented the use of three-dimensional prints of the patients’ skull that can demonstrate the bony defect (Figure 3).”
Surgical process
Following careful preoperative set-up, including facial nerve monitor, the surgery begins with a postauricular approach and an anteriorly based periosteal flap. Temporalis fascia and temporalis muscle grafts are then harvested and preserved for future use in a damp gauze swab. Adequate exposure of McEwan’s triangle is required, with identification of bony landmarks: posterior root of zygoma, spine of Henle, mastoid tip, and temporal crest.
Typically, a cortical mastoidectomy is performed, ensuring tegmen mastoideum, sigmoid sinus and sinodural angle are delineated. Some bone dust is harvested at this stage and mixed with a non-ototoxic antibiotic (bone pâté) for use as further graft material. If improved access is required, the sigmoid sinus can be partially exposed with the use of a diamond burr, allowing retraction of the sinus posteriorly. Mastoid air cells are removed and the mastoid antrum is opened until the short process of the incus and the lateral semicircular canal are clearly visible, with the second genu of the facial nerve located inferior to the midpoint of the canal. The facial nerve can also be identified in the tympanon but also within the mastoid bone.
Perilabyrinthine air cells superior to the lateral semicircular canal are removed until the posterior semicircular canal is well identified. The superior semicircular canal is identified anteriorly close to the anterior aspect of the lateral semicircular canal (Figure 4) and then carefully followed posteriorly towards the common crus of the superior and posterior semicircular canals. The superior semicircular canal can now be exposed anteriorly and posteriorly, with dissection extending towards the middle fossa dura. As the middle fossa dura is approached, care should be taken to prevent injury and cerebrospinal fluid leak.
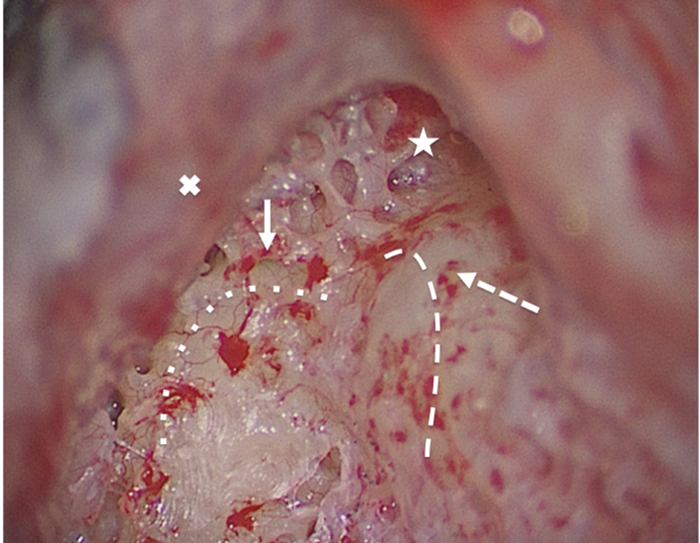
Figure 4. The approach to the superior semicircular canal obliteration in a right ear: the star shows the antrum, the X shows the skeletonised, but not exposed, middle fossa dura; the white arrow points the anterior aspect of the superior and the dashed white arrow the anterior aspect of the lateral semicircular canal. The route of the superior and the lateral canals are highlighted with a dotted and dashed line, respectively.
‘Blue lining’ of the superior semicircular canal is performed at its anterior and its posterior end until the endosteum is clearly visible without, however, breaking through it to prevent any perilymph leak (Figure 5). In case of a leak, additional care should be taken with the suction to avoid inner ear trauma. The ‘blue lining’ of the semicircular canal is better and safer performed with a 2-3 mm diamond burr under thorough irrigation to avoid high temperatures and thermal damage to the inner ear.
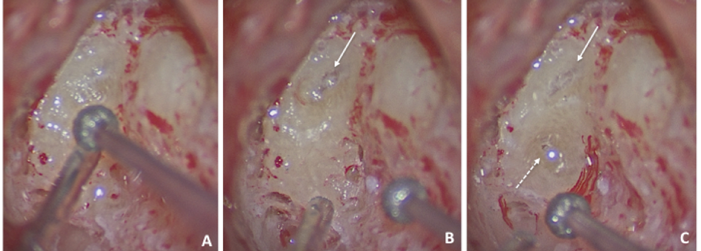
Figure 5. The anterior aspect of the superior semicircular canal is gradually ‘blue lined’ (A) until the endosteum is visibl e- white arrow (B); the same process is followed for the posterior aspect of the superior canal-dashed arrow (C).
After adequate exposure, the superior canal is plugged in its posterior and anterior end very slowly with small pieces of muscle (Figure 6) and covered by fascia and by bone pâté (Figure 7) to ensure a robust obliteration. The use of bone pâté directly through the ‘blue lined’ defect or even over the muscle is not recommended, in case small bony particles escape into the labyrinth causing significant dizziness. The superior semicircular canal should ideally be obliterated in two sites, one anteriorly and one posteriorly to ensure complete obliteration of the canal (Figure 5); obliterating only on one site can, in theory, cause abnormal perilymph flow and dizziness, although such technique has never been used by the authors.
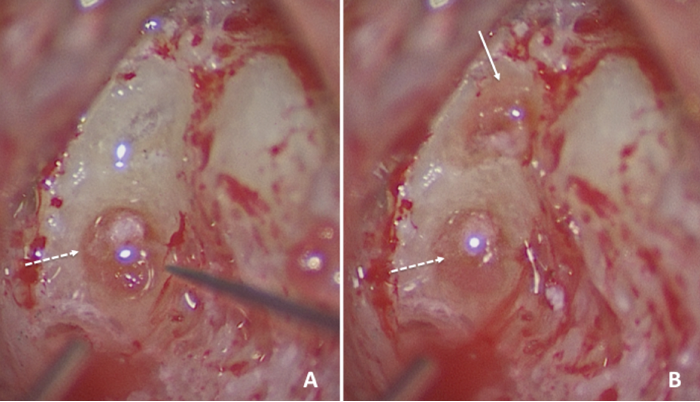
Figure 6. Both ends of the superior semicircular canal are obliterated with muscle (posterior end-dashed arrow A and anterior end-white arrow B).

Figure 7. Both sites are covered with fascia (marked with X, A) and then with bone pâté (B).
The operation ends with wound closure in layers. The patient is usually kept in overnight, to ensure the absence or adequate control of acute vertiginous symptoms, if any. Typically, the facial nerve function is checked postoperatively, as well as the inner ear function (spontaneous nystagmus and lateralisation of Weber’s test). Of note, fine beating nystagmus to the ipsilateral side is expected, given the temporary ‘irritation’ of the operated inner ear; this usually settles within a couple of hours postoperatively.
The patient is reviewed in the neurotology clinic in three weeks and three months postoperatively; the audiovestibular assessment is also repeated to document progress/recovery.
Short discussion
The trend in the surgical management of SSCD has recently been in favour of the transmastoid approach over the middle cranial fossa approach. This is due to the procedure having a good safety profile, equivalent efficacy and shorter hospital stays in comparison to the middle cranial fossa approach [5]. Furthermore, as the middle cranial fossa approach involves brain retraction and dural exposure the potential for serious complications is higher [6].
“The use of bone pâté directly through the ‘blue lined’ defect or even over the muscle is not recommended, in case small bony particles escape into the labyrinth causing significant dizziness.”
The authors of this paper also advocate canal plugging over resurfacing techniques, despite the theoretically increased risk of mild sensorineural hearing loss, due to the usually straightforward approach and the improved procedure success rates [7].
The standardised preoperative work out including audiovestibular tests (emphasis given to cVEMPs and six-canal vHIT) and the three-dimensional skull prints, the careful patient selection, the very detailed consultation about the patient’s realistic expectations and the fine surgical technique described above, result in favourable outcomes, with the potential to significantly improve the patient’s quality of life.
References
1. Minor LB, Solomon D, Zinreich JS. Sound- and/or pressure-induced vertigo due to bone dehiscence of the superior semicircular canal. Arch Otolaryngol Head Neck Surg 1998;124(3):249-58.
2. Belden CJ, Weg N, Minor LB, Zinreich JS. CT evaluation of bone dehiscence of the superior semicircular canal as a cause of sound- and/or pressure-induced vertigo. Radiology 2003;226(2):337-43.
3. Milojcic R, Guinan JJ Jr, Rauch SD, Herrmann BS. Vestibular evoked myogenic potentials in patients with superior semicircular canal dehiscence. Otol Neurotol 2013;34(2):360-7.
4. Zuniga MG, Janky KL, Nguyen KD, et al. Ocular vs. cervical VEMPs in the diagnosis of superior semicircular canal dehiscence syndrome. Otol Neurotol 2013;34(1):121-6.
5. Rodgers B, Lin J, Staecker H. Transmastoid resurfacing versus middle fossa plugging for repair of superior canal dehiscence: comparison of surgical techniques from a retrospective cohort. World Journal of Otolaryngology Head & Neck Surgery 2016;2(3):161-7.
6. Chilvers G, McKay-Davies I. Recent advances in superior canal dehiscence syndrome. J Laryngol Otol 2015;129(3):217-25.
7. Vlastarakos PV, Proikas K, Tavoulari E, et al. Efficacy assessment and complications of surgical management of superior semicircular canal dehiscence: a meta-analysis of published interventional studies. Eur Arch Otorhinolarygol 2009;266(2):177-86.




