In this article, the authors describe the retrosigmoid approach to a vestibular schwannoma, using an ultrasonic bone aspirator as an alternative to the standard drill.
Vestibular schwannomas (VS) are benign, usually slow-growing tumours of the vestibular nerve. Management of VS consists of observation, stereotactic radiation therapy or surgical excision. Surgical excision is generally preferred in larger tumours and / or younger patients, although there are not any universally agreed indication criteria.
There are three main surgical approaches to excision of VS; translabyrinthine, retrosigmoid and middle cranial fossa [1]. The retrosigmoid approach is suitable for a vestibular schwannoma (VS) of any size, especially when there is typically minimal distal internal auditory meatus (IAM) extension. In selected cases, this approach can also allow for hearing preservation [1,2]. In this approach, the IAM is drilled to allow exposure of the nerves and the intrameatal part of the VS. This allows adequate access, identification and preservation of the facial nerve with tumour resection.
Traditionally, a high-speed drill has been used for the drilling of the IAM. While well-tested, drills can cause bone dust to accumulate in the subarachnoid space, which is thought to contribute to postoperative headaches. Additionally, their use introduces a high-speed power instrument into the intracranial cavity.
"While well-tested, drills can cause bone dust to accumulate in the subarachnoid space, which is thought to contribute to postoperative headaches"
Recently, the evolution of ultrasound-powered tools has resulted in aspirators that can be used not only on soft tissues but also on bone. These tools use ultrasonic vibration to emulsify bone and provide suction and irrigation simultaneously in one single device, which results in minimum amount of bone dust. Such devices could provide an alternative to power drills for ‘drilling’ the IAM in the retrosigmoid approach.
Technical description
The authors describe the retrosigmoid approach utilising an ultrasonic bone aspirator (Sonopet® from Stryker, Kalamazoo, Michigan, US) with the Long Spetzler Micro Claw tip for removing the IAM bone [3]. The preparation for the procedure and the retrosigmoid craniotomy take place in the usual manner, which is outside the scope of this paper [1,2].
In summary, following careful positioning of the patient, the facial nerve monitor is set up and the patient is prepped and draped as per local standards. The mastoid tip and digastric groove provide anatomical landmarks for identifying the sigmoid sinus. A C-shaped incision is made in the retro-auricular region through skin and soft tissue and a subperiosteal flap is elevated. A burr hole is made at the junction of the transverse and sigmoid sinuses, at the edge of the posterior mastoid notch. A perforator and craniotome are used to elevate a bevelled bone flap and the bony window is enlarged as required. The posterior edge of the sigmoid sinus can be visualised at the anterior edge of craniotomy; this allows adequate access. A U-shaped incision is made in the dura, the inferior cistern is drained of CSF and dura is retracted towards the sinus. The cerebellum is gently retracted to allow for visualisation of the cerebellopontine angle and access to the VS.
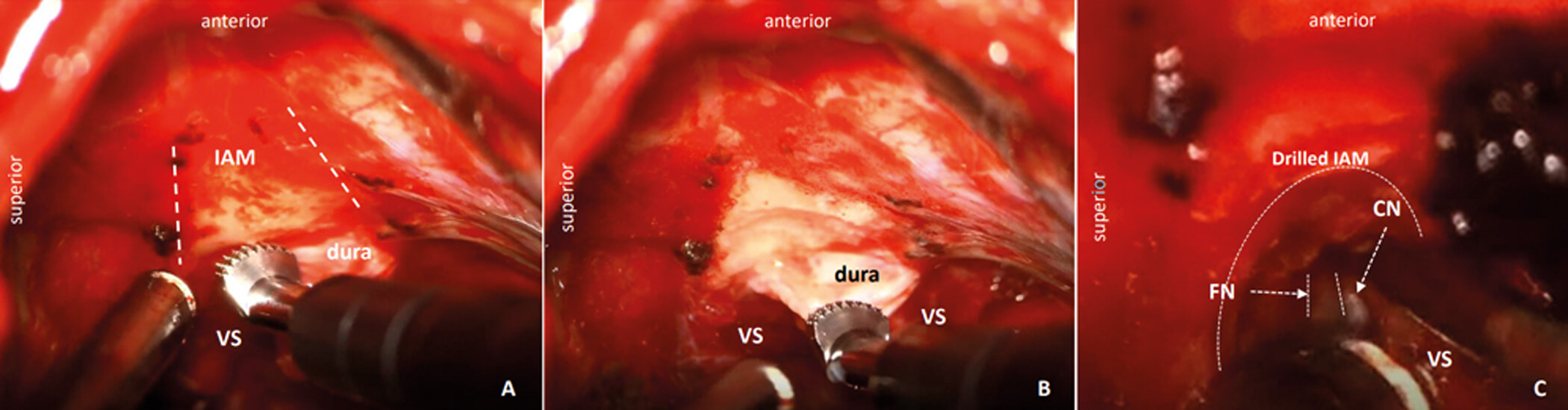
Figure 1: A) Intraoperative images of a right-sided VS resection, showing the tip of the ultrasound bone aspiration with the micro claws, with the area of the IAM marked (dashed lines); B) The bone of the IAM is gradually removed, while the dura remains intact; C) The exposure allows identification of the facial nerve (FN – dotted lines) in the IAM, while the cochlear nerve (CN) is also identified. The curved line shows the IAM area of removed bone.
Arachnoid dissection is carried out; depending on the tumour size, central debulking using the soft tissue tip of the ultrasound aspirator is utilised in a staged manner until the facial nerve and the eighth cranial nerve are identified at their origin at the brainstem. At this point, the tumour is followed towards the IAM, which will require bone removal to access the intrameatal part of the VS and to identify the facial nerve distally. Dura overlying the temporal bone is dissected to prepare for ‘drilling’ of the temporal bone to access the IAM. The ultrasonic bone aspirator is used to ‘drill’ out the IAM in a staged manner (Figure 1). Care is taken to avoid entering petrous apex air cells (avoid postoperative CSF leak / rhinorrhoea). Once satisfactory access to the IAM contents is achieved, the facial nerve in the IAM is identified and the VS resection is finalised, with careful dissection and separation of the facial nerve from the tumour (Figure 1). At the end of the procedure, following removal of a small amount of bone from the IAM, resection of even a large VS with facial nerve preservation is achieved (Figure 2).
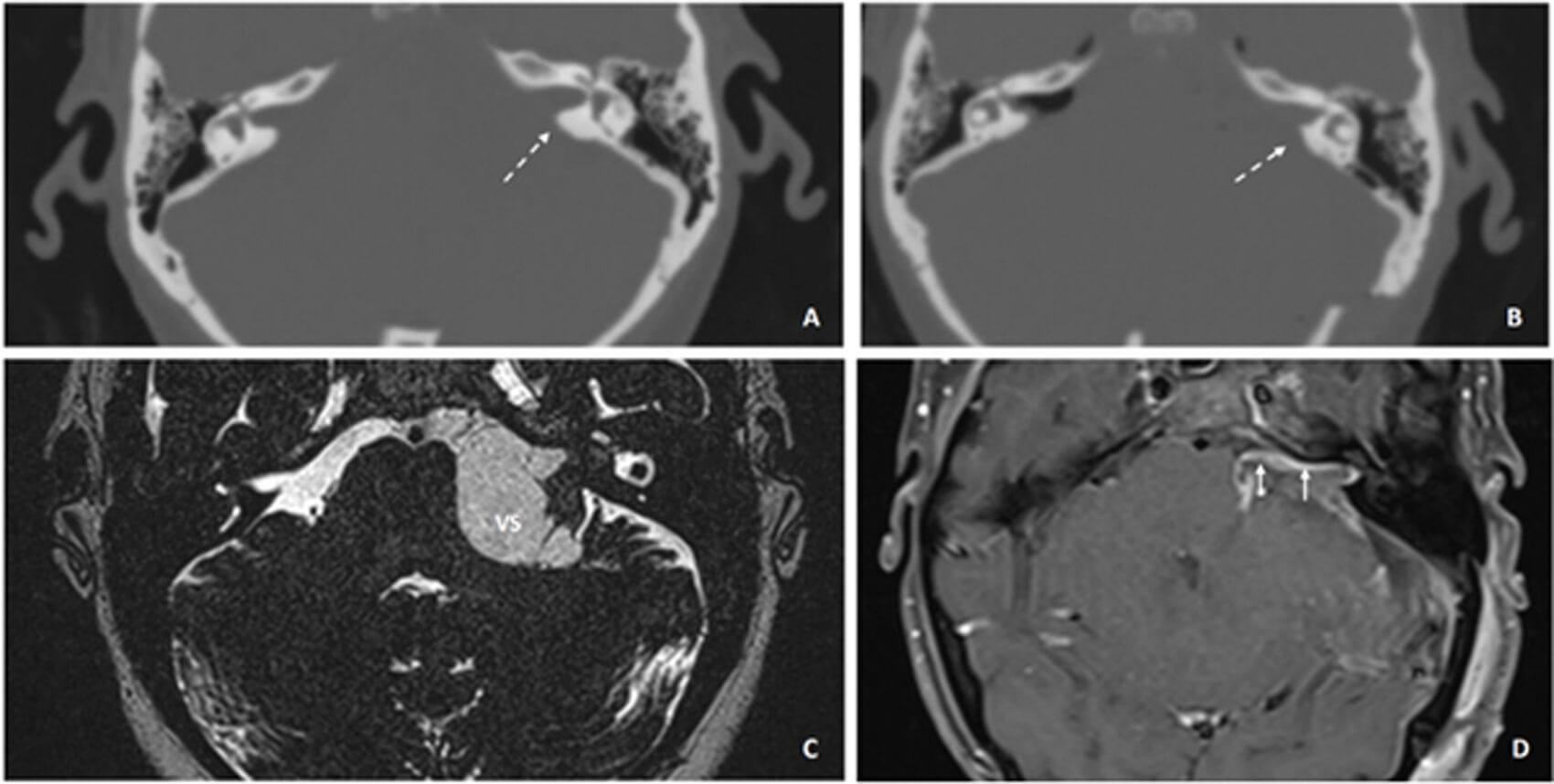
Figure 2: Preoperative computed tomography (CT) of the temporal bones: A) of a patient with a large left VS; and B) the postoperative scan showing the area of the bone of the IAM that has been removed, highlighted with dashed arrows. C) The magnetic resonance imaging T2-weighted steady state shows the large VS preoperatively; and D) postoperatively (day three) on post-gadolinium T1-weighted MRI. The short arrows highlight the postoperative enhancement along the whole route of the facial nerve.
Haemostasis is achieved with a combination of low-powered bipolar diathermy and use of haemostatic agents. The craniotomy is closed in a usual, in-layers manner.
Discussion
The authors present an adaptation of the retrosigmoid approach to VS, using an ultrasonic bone aspirator rather than a standard drill for IAM ‘drilling’. In craniofacial surgery, ultrasonic bone aspirators are used widely and recognised for the reduction in bone dust and safe use in areas with limited surgical access [4]. In the authors’ experience, this instrument allowed for effective temporal bone ‘drilling’ and with a reduction in the production of bone dust. It has been proposed that postoperative headache following craniectomy may be a result of meningeal irritation from collection of bone dust in the subarachnoid space, but there is conflicting evidence in the literature as to the aetiology of postoperative headache after the retrosigmoid approach [5]. The authors report the ultrasonic bone aspirator is slower than a standard drill, but the area of drilling is so reduced that speed does not significantly add time to an overall lengthy operation. To fully establish the benefits of the ultrasonic bone aspirator compared to the standard drill, further research is required. In the authors’ practice, the ultrasonic bone aspirator is a safe, easy-to-use instrument that is effective in ‘drilling’ the IAM in the retrosigmoid approach for VS resection.
References
1. Alomari AA, Campione A, Iavarone S, et al. Optimizing retrosigmoid approach for giant vestibular schwannoma resection: strategies and advances in surgical technique. AME Surg J 2024;4:1–9.
2. Corrivetti F, Cacciotti G, Scavo CG, et al. Flexible Endoscopic-Assisted Microsurgical Radical Resection of Intracanalicular Vestibular Schwannomas by a Retrosigmoid Approach: Operative Technique. World Neurosurg 2018;115:229–33.
3. Weber JD, Samy RN, Nahata A, et al. Reduction of bone dust with ultrasonic bone aspiration. Otol Neurotol 2015;152:1102–7.
4. Daly GE, Luh RA, Balumuka D, et al. The Sonopet iQ® Ultrasonic Bone Aspirator in Craniofacial Surgery: A Scoping Review and Qualitative Analysis. Face 2024;5:261–71.
5. Ren Y, McDonald MA, Manning P, et al. Dispersed bone spicules as a cause for postoperative headache after retrosigmoid vestibular schwannoma surgery: A myth? J Neurol Surg Skull Base 2022;83:374–82.
Declaration of competing interests: None declared.




