![]()
John Fenton, Republic of Ireland, has recently been appointed President of the Union Européene Des Médicins Spécialistes (UEMS) ORL or European Union of Medical Specialists ORL Section. We caught up with him to find out a little more about his own training, the principles of the UEMS, and of course, Brexit.

Professor John Fenton.
Congratulations on your Presidency of UEMS ORL; can you tell us a bit about how you came to this position?
There are a number of strings to my bow including tradition, birthright, experience and ‘Europhilia’, which have resulted in my appointment as president of this august body.
I originate from an Irish-speaking district of County Kerry on the southwestern seaboard of Ireland and my home town of Dingle has had centuries of marine trade with Europe. Excluding Iceland and islands such as the Canaries or the Azores, it is the most westerly point in Europe with next stop the USA. Natives of this region of Desmond which is the ancient Irish territorial division of South Munster, were granted citizenship of Spain by King Phillip II of Armada fame (or notoriety depending on one’s outlook) in the 1500s. The son of a wine merchant whose residence still stands on the street that I grew up on was an officer in the Austrian army and also aide-de-camp to Marie Antoinette in Paris before her unfortunate demise by guillotine. Plans were afoot to smuggle her by sea to safety in Dingle but she refused to leave her husband. There are Spanish markings from the 17th Century on two houses close to my family home and one of the local churches is named after the Gallician Camino pilgrimage destination of Santiago de Compostelo, which was accessed by sea for hundreds of years by denizens of Daingean Ui Chuis (Gaelic for Dingle).
In the past 50 years, especially since the David Lean film, Ryan’s Daughter, the Dingle Peninsula, or Corca Dhuibne, which is renowned for its spectacular scenery, has evolved into one of the foremost tourist destinations in Ireland. It also has a busy working fishing harbour used by many European trawlers while yachts from all over the world avail of its amenities and safe shelter. As a child or teenager growing up there, the holiday season was quite cosmopolitan with approximately a quarter of visitors German, a quarter British, a quarter comprising a miscellany of other nationalities and the remainder Irish. It is not surprising therefore that my outlook is to Europe and beyond, notwithstanding the price that the Irish fishing industry had to and still has to pay for entry into the EEC.
My specialty training was mainly in Ireland and I was fortunate to obtain a fellowship or ‘assistant étranger’ position in Paris, France under the tutelage of Professors Jean-Marc and Olivier Sterkers after I had completed a similar operating attachment with Professor Paul Fagan in Sydney, Australia. My first consultant post was as senior lecturer at University Hospital Aintree and the University of Liverpool, UK, where Ray Clarke and Professor Andrew Jones persuaded me to take responsibility for postgraduate teaching in the Mersey Deanery. On my return to Ireland in 2001, I was instrumental in helping to set up the first Medical School in Ireland since 1854 at the University of Limerick and I was also involved in the introduction of a graduate-entry speech therapy Master’s degree course at that institution. At the same time, in conjunction with my now-retired ENT colleagues Peadar Keogh and Kevin Manning, we became the first department outside Dublin to be recognised by SAC/RCSI for three SpR training posts. I started the facial plastics surgical course for trainees with Mr Manning in Limerick and it immediately gained RCSI acceptance on the National Training programme, becoming an integral part of the annual calendar to this day.
“There are a number of strings to my bow including tradition, birthright, experience and ‘Europhilia’ which have resulted in my appointment as president of this august body.”
I instigated the Head and Neck section of the Annual Sylvester O’Halloran surgical meeting in 2005 which was the first time that our specialty had a formal presence at one of the more prestigious general surgical meetings in Ireland. It has developed into a relatively gentle forum for fledgling junior doctors and medical students taking their first steps in scientific presentations. I have been an intercollegiate examiner for the past five years and I am also an examiner at the annual EBR-ORL HNS specialty oral examinations in Vienna. Despite my training in lateral skull base surgery and head and neck oncologic surgery, I would now be considered a dinosaur or generalist with an academic bent. My international peer-reviewed publications tend to be clinical enquiries across the spectrum of our specialty but also involve an educational subset including what I deem my ‘esoteric academics’.
My colleagues at the Irish Institute of ORL-HNS elected me as their representative to the UEMS ORL section joining delegates from 33 countries primarily to harmonise specialty training in these nations. When the previous extremely hard-working, eminently obliging and exceptionally capable president of the UEMS ORL, Professor Ulrik Pedersen of Denmark decided to retire from the post in mid-2017, I was approached by the board as their unanimous nominee for the position. I was delighted to accept the invitation and was duly elected, with the specific support of my Irish colleague Professor Rory McConn-Walsh, and by my peers at our annual congress in Warsaw during October 2017.
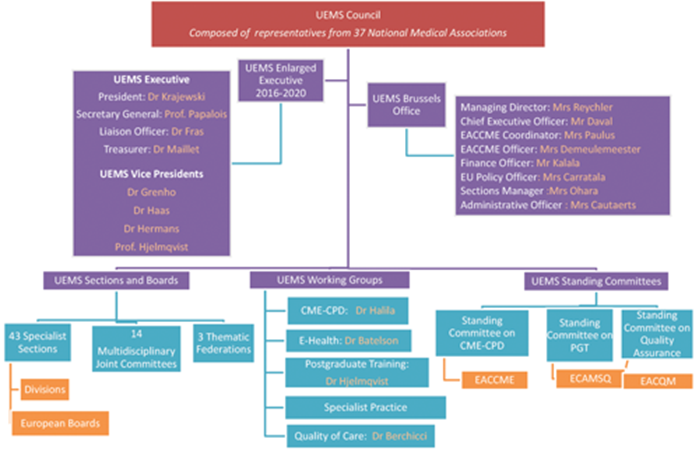
Figure 1. UEMS Council.
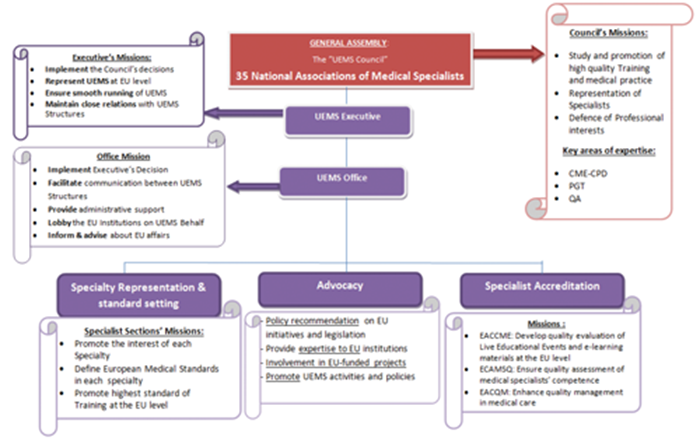
Figure 2. General Assembly of UEMS Council.
What are the principles of the UEMS ORL?
The Union Européenne des Médecins Spécialistes is the legal body representing medical specialists in Europe and is answerable to the Ministers of Heath within each jurisdiction. Its main function is to set standards for medical practice and harmonise them throughout the European Union, while providing representation of medical specialists to the European Commission. The general body of the UEMS is composed of national associations (NMAs) that represent medical specialists in 40 countries (Figures 1-2) and a strategy for the future is outlined in Table 1. There are 31 full member European states with four associates (Armenia, Israel, Serbia, Turkey) and five countries classified with observational status (Georgia, Iraq, Lebanon, Morocco, Tunisia). Of note with regard to Brexit, 28 of these countries are currently in the EU, while three are within Europe but outside the formal concord (Iceland, Norway, Switzerland).

UEMS-ORL (otorhinolaryngology) is one of the 43 sections within the UEMS family. The role of the UEMS-ORL is to define and harmonise ORL training programmes in Europe. There are fewer member countries in the ORL cohort than in the general group which comprises the current EU 28, Norway and Switzerland as full members while Turkey and Serbia are associates with Bosnia as the sole observer state. Several full member countries have been less than forthcoming with annual fees and are hanging on by their coat-tails. Typically each country’s medical association nominates one delegate from a professional and one from an academic background. Delegates meet annually in different locations on a rotational basis to primarily propose, update and set standards for training programmes in our specialty which are then addressed, recommended or implemented throughout the year by or under the instruction of the board.

Figure 3: (L-R) Ulrik Pedersen, Denmark (immediate Past President);
Wolfgang Luxenberger; Austria; Maria de la Mota, Spain; Adrian Agius, Malta and myself.
The UEMS-ORL board (Figure 3) is comprised of the President, General Secretary (Adrian Agius, Malta) and Treasurer (Wolfgang Luxenberger, Austria) who fulfil a four-year term with an option of a further four years extension if acceptable, while the permanent secretary (Maria de la Mota, Spain) looks after the day-to day administration and record keeping. The post of permanent secretary is the only one which is remunerated. The UEMS-ORL has established a competency-based logbook which trainees in all countries are encouraged to use for general otorhinolaryngology. The logbook was updated at the board meeting in Warsaw in October 2017. UEMS-ORL has in recent years compiled programmes for subspecialty training in head and neck, rhinology and otology / otoneurology with criteria for approved centres for such subspecialty training. The UEMS-ORL has close ties with the Confederation for European ORL (CEORL) which has sponsored one year European training fellowships in these areas. Recent years have seen the introduction of the European Board examination in ORL (EBE-ORLHNS) which is increasing in popularity and is taken by many European and non-European candidates.
Success in the examination does not guarantee a working position in Europe but confirms that the candidate reaches a certain standard. The examination is made up of a first written part (multiple choice questions) and an oral second part. The oral examination takes place in November and brings together approximately 70 experienced examiners from all over Europe, therefore ensuring a truly inclusive dimension to the EBE-ORLHNS.
How does an impending Brexit look from the European side?
Generally, from a continental, mainland or for accuracy, should I say non-British perspective, the result was considered quite a surprise, but personally with my first-hand knowledge of the electorate, I managed to predict the outcome although I was not brave enough to bet on the result. The consensus is disappointment with the outcome but that it was a vote by the British people for the British people and they will have to live by their democratic decision whichever way it evolves. The feeling from an international UEMS aspect is that it will probably not impact on the vast majority of trainees in Europe but could have implications for Irish medical graduates who often further their careers on our neighbouring island. If I don my colloquial hat, I do not envisage any disruption to the IOS annual conference which is our most prestigious scientific meeting and a joint venture between the specialty in the Republic of Ireland and The North.
“The role of the UEMS-ORL is to define and harmonise ORL training programmes in Europe.”
There has been admirable cross-border cooperation in patient care with the support of European funding and this is one of the few relevant healthcare worries that exist on our north-western outcrop. There is an old Irish adage that Ireland and England are like a married couple whereby ‘they fight all the time but don’t try to get between them’! This domestic arrangement will probably have to change in some way and the other well-known saying that ‘the English never remember and the Irish never forget’ may come into play, particularly as our priority outside of medicine must be maintaining the peace accord and that nothing should be allowed to compromise the delicate equilibrium that has existed in recent years.
At our section meeting in Prague 2016, Tristram Lesser and Brian Bingham expressed their opinion that Britain would continue to be active participants of the UEMS and that, considering the makeup of UEMS ORL, Brexit overall was unlikely to make a difference to the policies of the group. There is an extraordinary contribution from British colleagues to the EBE-ORLHNS examinations and the hope is that these efforts will not only continue but flourish no matter what happens following Brexit. Likewise the formulation and launch of a surgical logbook to encompass all member countries will still be available to all. An ongoing bone of contention is that our attempts to legally change our formal European title to incorporate head and neck surgery have been vehemently opposed to by a British surgeon in a ’sister’ specialty, so it is possible that Brexit in some way may diminish his influence in Brussels. We do not claim ownership to the addendum and are quite happy for other disciplines such as endocrine or general surgery to utilise the same designation, especially if they can match our training programmes, research output, logbook requirements and examinations.
How do you foresee that Brexit might affect the European medical workforce?
It may alter the easy freedom of travel for service and training delivery, so considering that a notable percentage of junior doctors in Britain are from the EU but much less so in reverse, it implies that future developments are likely to have more of an impact on the British workforce than the European one. It may well however reopen up the Commonwealth supply corridor resulting in a personnel-neutral outcome. There may be a loss of European funding opportunities in surgical research for British trainees but overall Brexit is not perceived as a significant concern for the grassroots of European ORL-HNS that we represent.
Finally – what’s your favourite country, and why?
Excluding my own little piece of paradise on the south-west coast of Ireland, I would find it difficult to decide between my two fellowship destinations of Australia or France. The inherent attractions of both are obvious and I don’t absolutely subscribe to the concept of ’two beautiful countries, shame about the crowd who live in them!’ I love visiting both states for the eclectic experience of Oz and the admirable traditions of France, with fabulous life-long friends in each. If I have to choose it would be France, but only for ease of access. Joking aside and reverting to ORL-HNS for conclusion, I covet the methods and systems that have developed in both countries but most importantly the French concept of the predominantly medical ORL specialist which results in an almost complete lack of waiting lists. This according to most ‘experts’ is an unachievable dream but I thank you for allowing me to articulate it.



