This team of audiologists from Cincinnati Children’s Hospital Medical Centre discuss an eight year old with congenital CMV, a neonatal infection which is usually asymptomatic, and provide guidance on how to recognise the signs in the paediatric population, and screen for vestibular dysfunction.
The effects of congenital cytomegalovirus (CMV) on the brain and auditory system of newborns have been well documented [3]. Vestibular dysfunction due to CMV is less well understood but, nevertheless, exists. Bedside testing and a systematic case history will aid in appropriate referrals for vestibular assessments. Both hearing and balance should be routinely assessed in individuals with congenital CMV.
“Vestibular dysfunction associated with CMV is less recognised, partly due to a child’s inability to describe feelings of imbalance or vertigo, as well as parents mistaking symptoms of imbalance for clumsiness.”
What is CMV?
Cytomegalorivus (CMV) is a common herpes simplex virus that can be passed from mothers to babies during pregnancy, affecting 1% of all newborns. The majority (90%) of babies infected with CMV in utero are asymptomatic at birth, but later, about 20% show hearing or vision loss, seizures or other neurologic problems. Symptoms of an active infection at birth include jaundice, petechiae and hepatosplenomegaly. Both asymptomatic and symptomatic infants, however, may later develop health problems or disabilities. Currently, there is no vaccine to prevent CMV, so prevention during pregnancy and antiretroviral treatment in symptomatic infants is important.
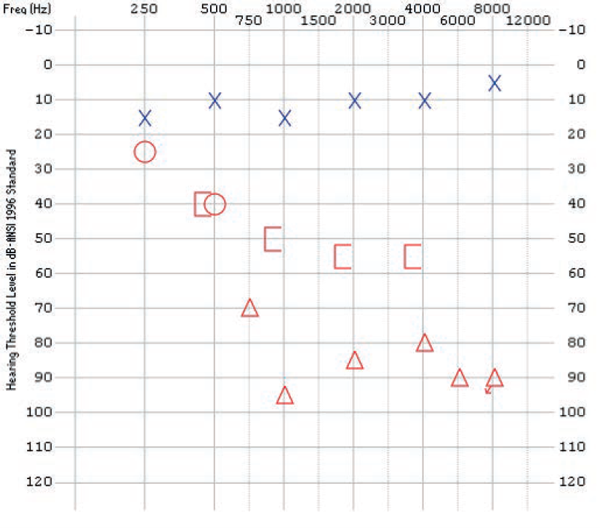
Figure 1: Audiogram of JW at 8.7 years of age indicating mild sloping to profound
mixed hearing in loss in the right ear and normal hearing in the left ear.
CMV and the inner ear
Sensorineural hearing loss is the most common auditory system finding. Sensorineural hearing loss may be present at birth or have a delayed onset. Hearing loss is usually severe to profound, is usually unilateral in asymptomatic CMV, bilateral in symptomatic CMV, of variable configuration and is often fluctuating or progressive [3].
“Cytomegalovirus (CMV) is a common herpes simplex virus that can be passed from mothers to babies during pregnancy, affecting 1% of all newborns.”
There is much less documentation of the effects of CMV on the vestibular system. Histological studies [2] confirm the presence of CMV in the vestibular portion of the inner ear, as well as the auditory portion, however vestibular dysfunction may exist with or without hearing loss and hearing loss may occur without balance dysfunction. Studies from the early 1980s and 1990s have reported variable presentations of vestibular dysfunction, not unlike the variable presentations of auditory dysfunction, related to CMV. Based on studies of post mortem temporal bones of infants with CMV, it is believed that vestibular dysfunction is a result of labyrinthitis of the endolymphatic system and disruptions in the sensory epithelia of the saccule and utricle. A handful of studies have indicated that caloric testing appears to be most likely to identify vestibular dysfunction due to CMV, followed by vestibular evoked myogenic potential testing (VEMP) [4,5,6]. We present here results of a case that illustrates the vestibular impact of congenital CMV.
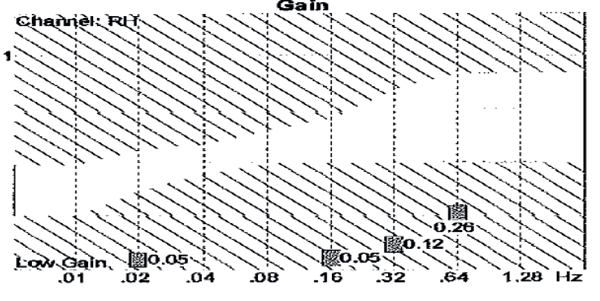
Figure 2: Sinusoidal harmonic acceleration testing revealed low gain across
multiple frequencies, suggesting bilateral peripheral weakness.

Figure 3: VEMP test results showing a normal response on the left and an absent response on the right.
CASE STUDY:JW
History
JW is an 8.7 year-old male who was born with congenital CMV. He has cortical visual impairment, developmental delays, cerebral palsy, seizure disorder, muscle weakness and spasticity.
Auditory assessments
Birth: Passed newborn hearing screening.
Six months: Diagnostic ABR due to risk for progressive loss.
- Left ear: Normal
- Right ear: Mild to moderate loss
Two years: Follow-up audiology – Normal responses in the sound field and a normal speech awareness threshold was obtained in both ears via insert earphones.
Eight years: A consultation with an otolaryngologist was sought for abnormal gait and balance concerns.
CT scan – Normal temporal bones with long-standing abnormal brain findings characteristic of perinatal CMV infection.
Audiogram (Figure 1)
- Right ear: Mild sloping to profound mixed hearing loss
- Left ear: Normal hearing
Vestibular evaluation
Sinusoidal harmonic acceleration: Low gain across several frequencies (Figure 2).
Step velocity testing: Limited responses in either direction.
Ocular motor evaluation: Unable to complete due to visual impairment.
Limited positional testing: No nystagmus in the pre caloric and neutral position.
Monothermal warm air caloric irrigation: No stimulated nystagmus in either direction.
VEMPs: Absent response on the right side with a normal VEMP on the left (Figure 3).
Summary
Consistent with a bilateral peripheral weakness.
Recommendation
Vestibular rehabilitation evaluation. Substitution exercises may strengthen the child’s other modalities to compensate for his lack of vestibular input to maintain balance. In addition, counselling regarding environmental modifications, such as well-lit hallways and removal of loose rugs to keep somatosensory input at a maximum will be beneficial.
Recognising the signs
The importance of obtaining routine hearing evaluations on children with CMV is universally accepted among health professionals. Vestibular dysfunction associated with CMV is less recognised, partly due to a child’s inability to describe feelings of imbalance or vertigo, as well as parents mistaking symptoms of imbalance for clumsiness. Consequently, health care professionals are less inclined to consider balance function when examining a child with CMV. As in the case of JW, however, CMV can become symptomatic through the first decade of life, affecting both hearing and balance.
Screening for vestibular dysfunction
If a child has a known diagnosis of CMV, the following questions may aid in identifying a potential candidate for vestibular testing.
- If over age three: Is your child clumsy? Does he/she frequently fall?
- Does he/she complain of spinning / dizziness / imbalance?
- Is there a history of delayed motor development?
- If age five or older: Can he/she ride a bike? Swim?
- Does he/she experience motion sickness or sensitivity?
- Have you ever seen your child’s eyes move back and forth quickly?

Figure 4 (left): Tandem Romberg. The child is asked to put one foot in front of the other, arms folded, then close eyes. The child should be able to maintain balance for 10 seconds. A fall to one side may indicate vestibular dysfunction. Note: The clinician is protecting the patient in the event of a fall.

Figure 5 (right): Head impulse test. The child is asked to stare at the sticker on the examiner’s nose while the examiner quickly moves their head to the right and then to the left. The examiner is looking for the child’s ability to maintain gaze on the sticker while the head is in motion. If the eyes move with the head and have to make a jump back to the sticker, this may indicate a peripheral vestibular weakness on the side to which the head was moved.
In addition, there are simple screening tests to supplement the case history that both clinicians and physicians can utilise in their office to determine if a referral for further testing is warranted. The Tandem Romberg (Figure 4) assesses the vestibular spinal reflex and the head impulse test (HIT) (Figure 5) assesses the vestibular ocular reflex (VOR). The combination of these easy to administer assessments in the office will help determine if a complete vestibular evaluation is warranted.
Summary
- CMV is a common neonatal infection that is typically asymptomatic.
- Congenital CMV is known to affect the auditory system, vestibular system, or both and is inconsistent in its presentation.
- Vestibular function should be routinely screened, along with vision and hearing, in children with a diagnosis of CMV.
References
1. Davis LE, Johnsson L, Kornfeld M. Cytomegalovirus labyrinthitis in an infant: morphological, virological, and immunofluorescent studies. J Neuropathol Exp Neurol 1981;40(1):9-19.
2. Gabrielli L, Bonasoni MP, Santini D, et al. Human fetal inner ear involvement in congenital cytomegalovirus infection. Acta Neuropathologica 2013;1(63). Available from http://www.actaneurocomms.org/content/1/1/63
3. Goderis, J, De Leenheer, E, Smets, K, Van Hoecke, H, Keymeulen, A, Dhooge, I. Hearing Loss and Congenital CMV Infection: A Systematic Review. Pediatrics 2014;134(5):972-82.
4. Huygen PLM, Admiraal RJC. Audiovestibular sequelae of congenital cytomegalovirus infection in 3 children presumably representing 3 symptomatically different types of delayed endolymphatic hydrops. Int J Pediatr Otorhinolaryngol 1996;35:143-54.
5. Pappas DG. Hearing impairments and vestibular abnormalities among children with subclinical cytomegalovirus. Ann Otol Rhinol Laryngol 1983;92:552-7.
6. Zagólski O. Vestibular-evoked myogenic potentials and caloric stimulation in infants with congenital cytomegalovirus infection. J Laryngol Otol 2008;122:574-9.
Declaration of competing interests: None declared.




