The human central auditory nervous system (CANS) is complex and highly dependent upon attention and cognitive brain regions. Profs David Moore and Harvey Dillon discuss novel assessment approaches to clarify auditory contributions to listening difficulties in children.
How can we separately assess CANS function from that of the ear, on the one hand, and from cognitive function on the other? With careful test design, it may be possible to measure auditory function separate from language, attention and memory. We will illustrate one method of achieving this, and show how identification of a specific deficit leads to deficit-specific remediation.
Separating CANS deficits from peripheral deficits
It may not be possible to isolate CANS from peripheral function using behavioural testing alone. Cochlear pathology can be extensive and complex, distorting neural signals and disrupting every aspect of CANS processing. While clearly dependent on the CANS, normal speech and binaural/spatial perception are also dependent on receiving signals of exquisite fidelity from both ears. It is desirable to be able to differentiate deficits in the CANS from deficits in the cochlea, because CANS deficits may be more plastic and therefore more likely than cochlear deficits to be amenable to remediation by training.
“How can we ensure that test scores outside the normal range reflect deficits in the CANS function being measured rather than deficits in language, attention or memory?”
Tests to detect peripheral deficits should include wideband reflectance (middle ear transmission), distortion product and transient evoked (click or chirp) OAE (mechanics and OHCs), audiometry from 0.25 to 16kHz (sensitivity), and click-train middle ear muscle reflexes (efferent reflex loops) [1]. Although incomplete, this list captures some currently measurable fundamentals of middle ear and cochlear function.
Separating CANS deficits from language, attention and memory deficits
To perform any behavioural test requires some attention and short-term memory ability. It also requires language ability, even if only to understand the test instructions. How then can we ensure that test scores outside the normal range reflect deficits in the CANS function being measured rather than deficits in language, attention or memory? There are two basic methods in use, which are described in the next two sections.
Language-free stimuli, with simple tasks
If the focus is on CANS function, rather than more generally on listening difficulties of whatever origin, test stimuli should use non-speech sounds. In some instances, however, speech sounds that have minimal language content, such as nonsense syllables, or consist of highly overlearned and simple language, such as the digits 0-9, are useful. A shortcoming of available tasks that use non-speech stimuli (e.g. gap detection, frequency discrimination, spectro-temporal discrimination) is that they require much simpler auditory processing operations than are needed to analyse and pattern recognise stimuli as complex as speech sounds. Tasks should use the smallest number of stimuli per trial to minimise memory. For example, dichotic testing with two pairs of sounds per ear (a commonly used test), a total of four stimuli to remember, produces test scores in children that are moderately correlated with verbal memory. Consequently, memory ability is probably affecting test scores, even when memory ability is well within the normal range [3]. The same task has also been shown to be related to attention [4].
Differential (or ‘derived’ or ‘subtractive’) testing
It is possible to design two very similar auditory tests that differ in just one auditory dimension (e.g. in timing, binaural or spectral cues). Assuming these two tests have very similar attention, memory and language demands, the difference between the test scores is highly affected by change in the auditory dimension, but is little affected by attention, memory and language abilities of the person being tested.
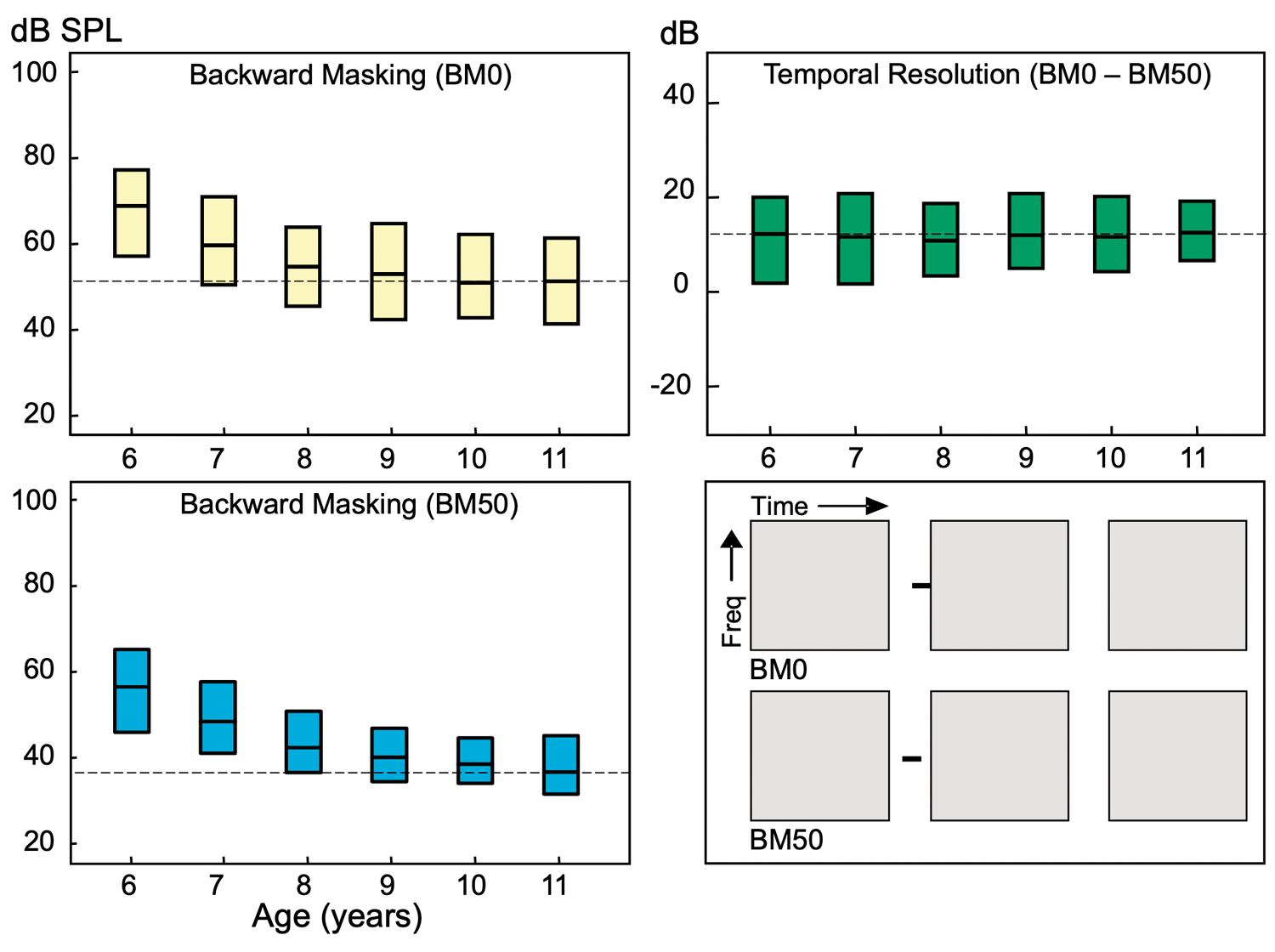
Figure 1. Differential testing for temporal resolution using auditory backward masking (BM). In these tests, three band-pass noises (gray boxes) are presented successively. Only one is preceded by a short tone (black line) and the listener must choose which one that is. Presented alone, tone thresholds for both the BM0 (yellow boxes; interquartile range, median) and BM50 (blue boxes) test decrease with age (6-11 y.o.). For the differential test (BM0-BM50, green boxes), temporal resolution does not change significantly across age. Adapted from Moore et al. 2010 [2].
As a first example, we can measure children’s ability to segregate sounds in time. One way to do this is to present a short (20ms) tone occurring immediately (BM0) or 50ms (BM50) before the noise (see Figure 1). In these separate tests that do not control for language, attention or memory, we see the typically reported maturity of hearing, with thresholds falling by 16-20dB between 6-11 years of age. By contrast, the difference in tone detection threshold (BM0 – BM50), a measure of auditory temporal resolution, remains steady at about 12dB across age. Temporal resolution may be sensitive to either a cochlear or CANS immaturity or abnormality, but is unlikely to be affected by a language, attention or memory deficit since those demands are very closely matched in the BM0 and BM50 tests.
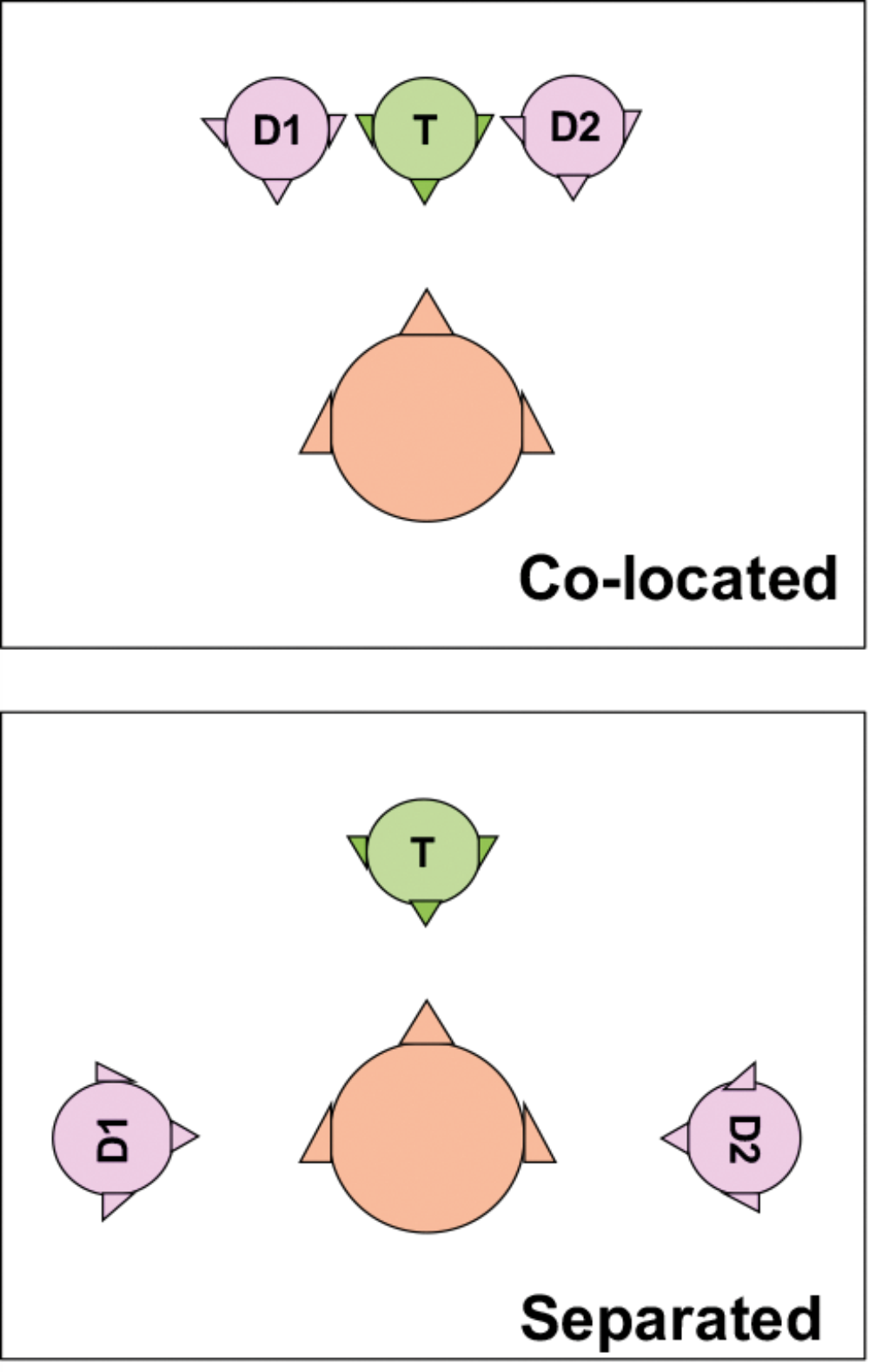
Figure 2. Differential test arrangement to diagnose a spatial processing disorder, as used in the Listening in Spatialized Noise Sentences test [6]. The target talker, T, is partially masked by the two distracting talkers, D1 and D2.
As a second example, we can measure a child’s ability to focus on target sounds from one direction, while suppressing sounds from other directions, by presenting target speech in a background of competing speakers, as shown in Figure 2. While language, attention and memory all likely influence the ability to understand speech in both the co-located and separated conditions, the difference in performance between the two conditions reflects primarily the child’s ability to use the spatial separation of sources to understand speech. Children who had multiple or protracted periods of middle ear infection during the first five years of life are many times more likely to have a deficit in this skill in later childhood, with consequent increased difficulty in understanding speech in situations with some background noise, like many classrooms.
“If the focus is on CANS function, rather than more generally on listening difficulties of whatever origin, test stimuli should use non-speech sounds.”
The differential procedure has a further advantage in that it enables very specific deficits to be identified. It seems likely that if a deficit can be identified as precisely as possible, remediation can be designed to enhance most efficiently the deficient skill. Certainly in the case of the spatial processing disorder referred to, deficit-specific training (LiSN & Learn, or its later version, Sound Storm) almost always enables children to attain normal spatial processing ability [5].
The disadvantage of differential testing is that because the final score is the difference of two base scores, there are two sources of random measurement error in the final score. This disadvantage has to be managed by test design that achieves suitably small random measurement error in each base score.
To summarise, it is not easy to separate the role that each part of the auditory system plays in hearing. Avoiding confounds of language, memory and attention just by keeping the stimuli language-free and the task as simple as possible is a worthy aim, but is not sufficient, at least with currently available tests, and in our opinion is never likely to be sufficient. But by using objective measures of ear function and differential behavioural testing of CANS function, we believe it is possible to draw out the role played by various parts of the system. This seems the best way forward in understanding and therefore in detecting and treating CAPD.
References
1. Valero MD, Hancock KE, Maison SF, Liberman MC. Effects of cochlear synaptopathy on middle-ear muscle reflexes in unanesthetized mice. Hear Res 2018;363:109-18.
2. Moore DR, Ferguson MA, Edmondson-Jones, AM, et al. Nature of auditory processing disorder in children. Pediatrics 2010;126(2):e382-90.
3. Cameron S, Glyde H, Dillon H, Whitfield J. Investigating the Interaction between Dichotic Deficits and Cognitive Abilities Using the Dichotic Digits difference Test (DDdT) Part 2. J Am Acad Audiol 2016;27(6):470-9.
4. Stavrinos G, Iliadou VM, Edwards L, et al. The Relationship between Types of Attention and Auditory Processing Skills: Reconsidering Auditory Processing Disorder Diagnosis. Frontiers in Psychology 2018;9(34).
5. Cameron S, Glyde H, Dillon H. Efficacy of the LiSN & Learn auditory training software: randomized blinded controlled study. Audiol Res 2012;2(1):e15.
6. Cameron S, Dillon H. The listening in spatialized noise-sentences test (LISN-S): comparison to the prototype LISN and results from children with either a suspected (central) auditory processing disorder or a confirmed language disorder. J Am Acad Audiol 2008;19(5):377-91.
Declaration of Competing Interests:
Professor Dillon is a part-time employee of the National Acoustic Laboratories (NAL). NAL, but not the author, receives royalties from the sale of LiSN-S, and revenue from the sale of Sound Storm.
David Moore gratefully acknowledges the support of the NIHR Manchester Biomedical Research Centre and Cincinnati Children’s Hospital Medical Center.
Harvey Dillon gratefully acknowledges the support of the NIHR Manchester Biomedical Research Centre and Macquarie University.




