
Manual audiometry has long been the gold standard for establishing hearing thresholds. In recent years, a number of automated audiometry applications have reached the market. In this article, a team from Ireland have put a version of automated audiometry to the test against the traditional method.
Background
Manual audiometry (MA) is the gold standard and primary means for diagnostic evaluation of hearing [1]. Quantifying hearing loss and determining the best amplification options for management of hearing loss are some of the main uses of MA. It is conducted by qualified audiologists, however audiologists are scarce in Ireland and access to services can be delayed. Patients are on long waiting lists for adult diagnostic hearing assessments and hearing aid fitting appointments. The average wait to avail a hearing assessment in a primary care centre or an acute hospital for a number of community health organisation areas within Ireland is approximately two years. However, a hearing test can be completed in aproximately 15-30 minutes.
The Automated Audiometry System (AAS) is a computer-assisted audiometer that allows users to self-administer their pure tone audiogram [2]. It can be operated by healthcare assistants who have undergone appropriate training with indirect support from audiologists.
The AAS has been validated for inter- and intra-rater accuracy and reliability in an NHS otology clinic setting [3]; as well as with ‘difficult-to-test’ patients with bilateral mixed, bilateral conductive, and unilateral conductive hearing losses [4]. AAS has been reported to be as reliable (within 10 dB) as audiologists at determining air- and bone-conduction hearing thresholds.
Despite its long history, a systematic review and meta-analysis has highlighted that validation is still limited for (i) automated bone conduction audiometry; (ii) automated audiometry in children and difficult-to-test populations, and (iii) different types and degrees of hearing loss [5].
The aim of this study was to validate AAS in an adult community audiology clinic and an acute ENT setting, for different types, degrees, and configurations of hearing loss. The two sites assess different patient cohorts particularly in terms of age and types of loss.
Given the reduced resources required to operate one or more AASs, it can be beneficial in improving access to audiological services in Ireland. It can enable redeployment of audiologists to clinical areas such as hearing aid fittings and complex caseload assessments that require more expertise.
Methods
Manual and automated audiometry were conducted at a Health Service Executive (HSE) adult community audiology clinic and a level 4 teaching hospital in Dublin, Ireland. Ethical approval was authorised by the MMUH Istitutional Review Board (Ref: 1/378/1928).
The participants were invited to undertake an AAS assessment as an additional investigation to MA, on the same day as their scheduled consultation. Queries with regards to the study were addressed and written consent was obtained.
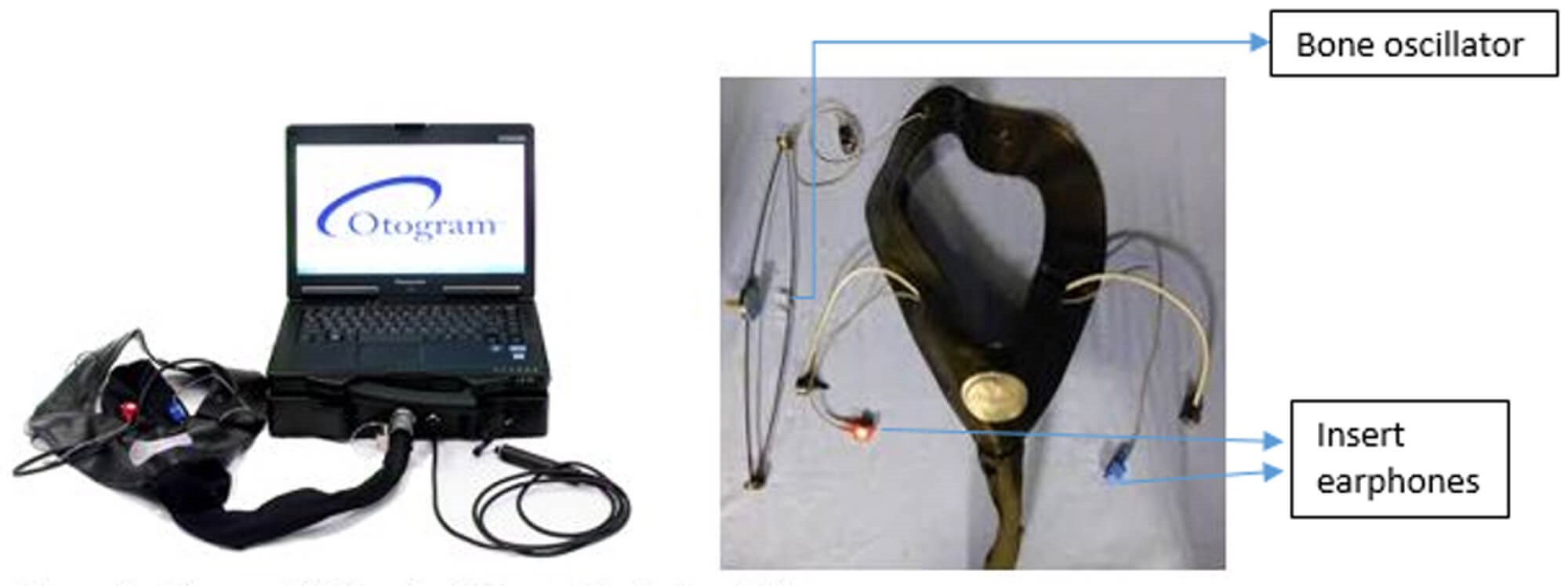
Figure 1. OtogramTM Hearing diagnostic system [2].
To ensure consistency, a trained healthcare audiology assistant administered the AAS testing, and was supported if required by an audiologist at both the community and acute sites. The OtogramTM Hearing Diagnostic System by Ototronix Diagnostics [2] was used (Figure 1). Participant selection and demographics for each site can be seen in Figure 2.
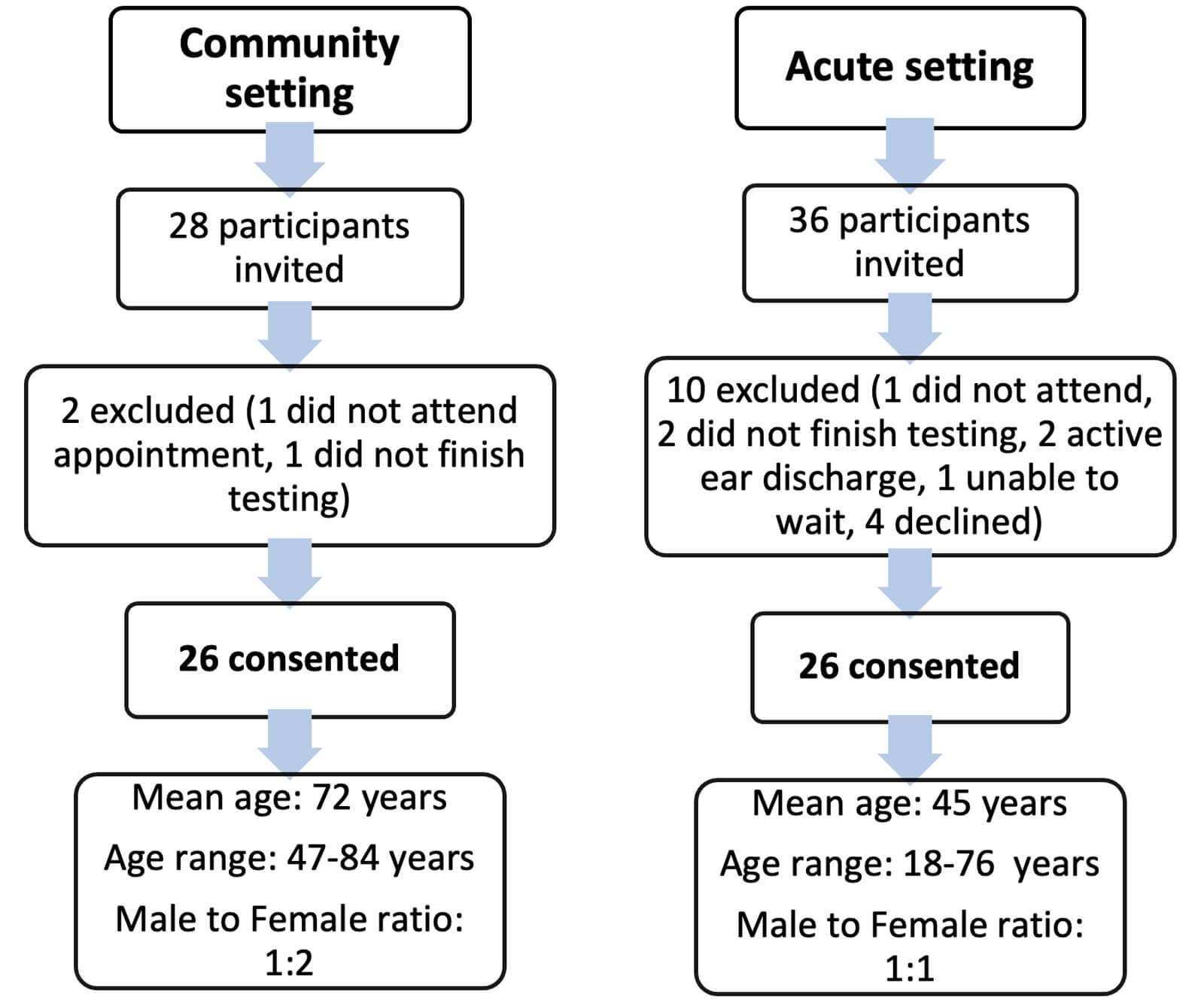
Figure 2. Participant selection.
Twenty six participants (52 ears) were tested using MA with TDH-39 headphones as per British Society of Audiology (2018) recommended procedure [1] and AAS via EAR-5A insert earphones in each of the two sites. Each centre divided their participants into equal subgroups of 13 participants performing MA first, followed by AAS and vice versa (Figure 3).
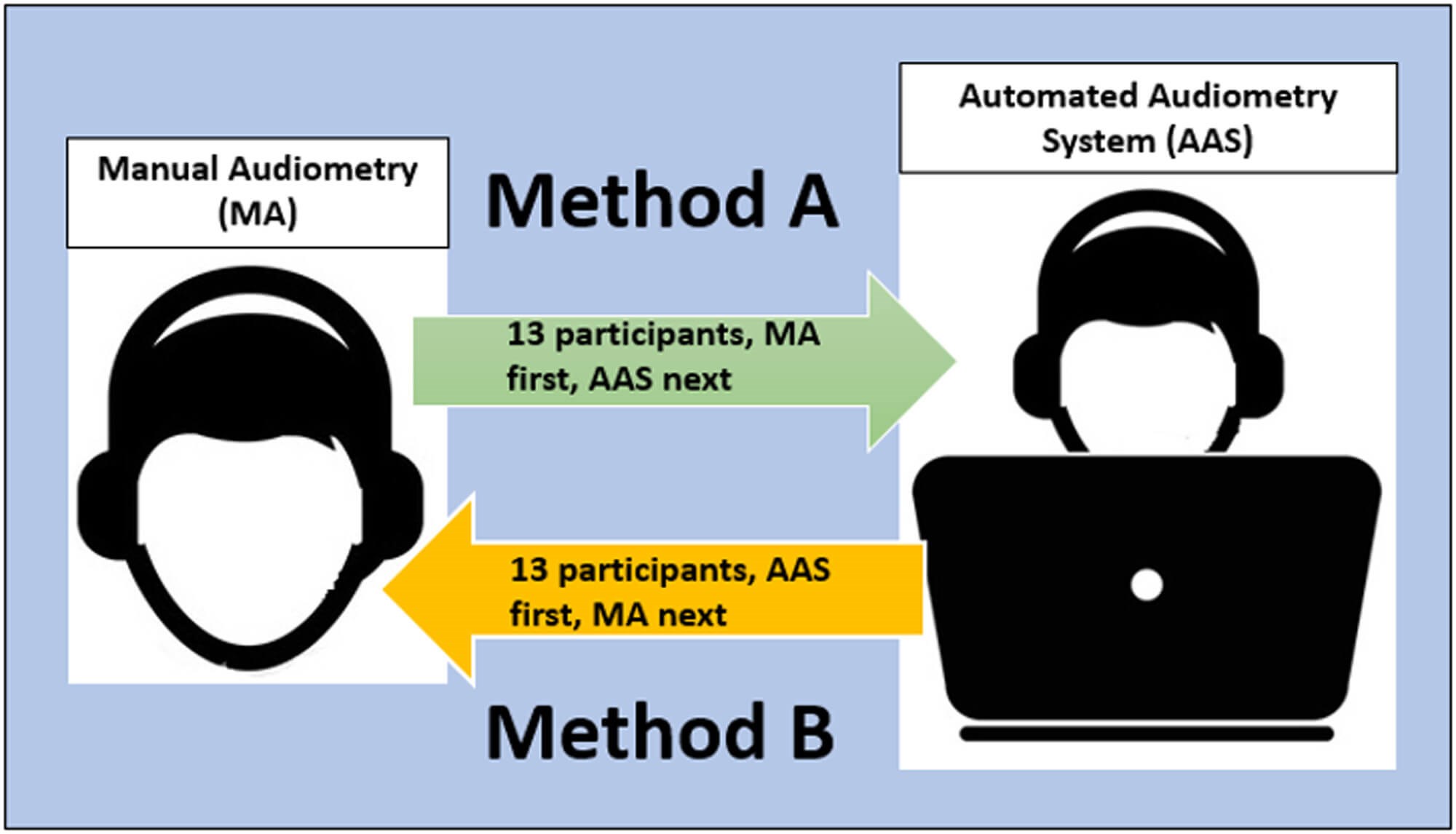
Figure 3. Methods A and B of testing. Each site performed MA first with 13 participants,
followed by AAS; and 13 participants performed AAS first followed by MA.
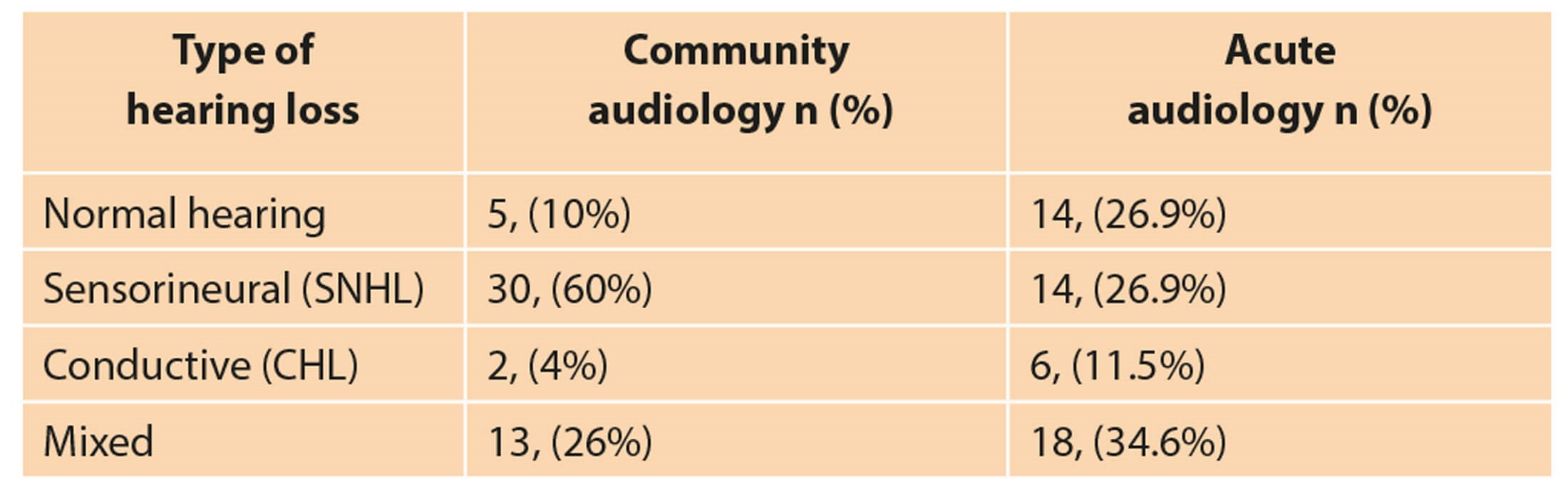
Table 1. Distribution - number (n) and percentage (%) - of ears tested in community and acute audiology setting.
Two ears in the community setting were not included in the above table, as bone-conduction testing was not done.
Results
Participants at the two sites had various types of hearing loss (Table 1). To compare the MA and AAS audiometry results, the average air (0.25-8 kHz) and bone (0.5-4 kHz) conduction thresholds were used for both the right and left ears.
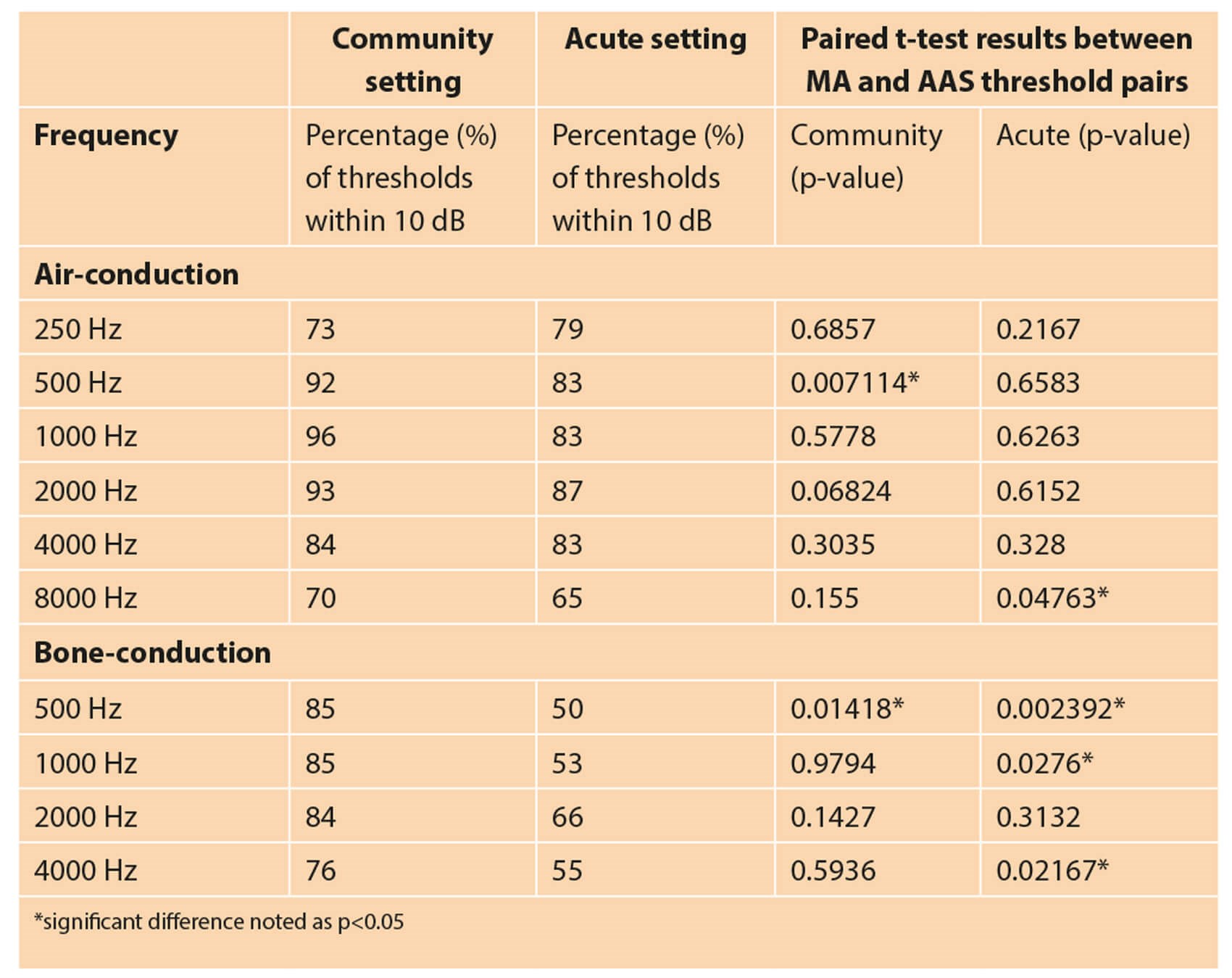
Table 2. Air- and bone- conduction threshold (including masked) comparisons between MA and AAS.
The results indicated that 70-96% of air-conduction, and 76-85% of bone-conduction thresholds obtained via AAS were within 10 dB of those obtained via MA when tested in the community setting; whereas 65-87% of air- and 50-66% of bone-conduction thresholds were within 10 dB in the acute setting (Table 2). A difference within 10 dB is considered an acceptable range of deviation [3].
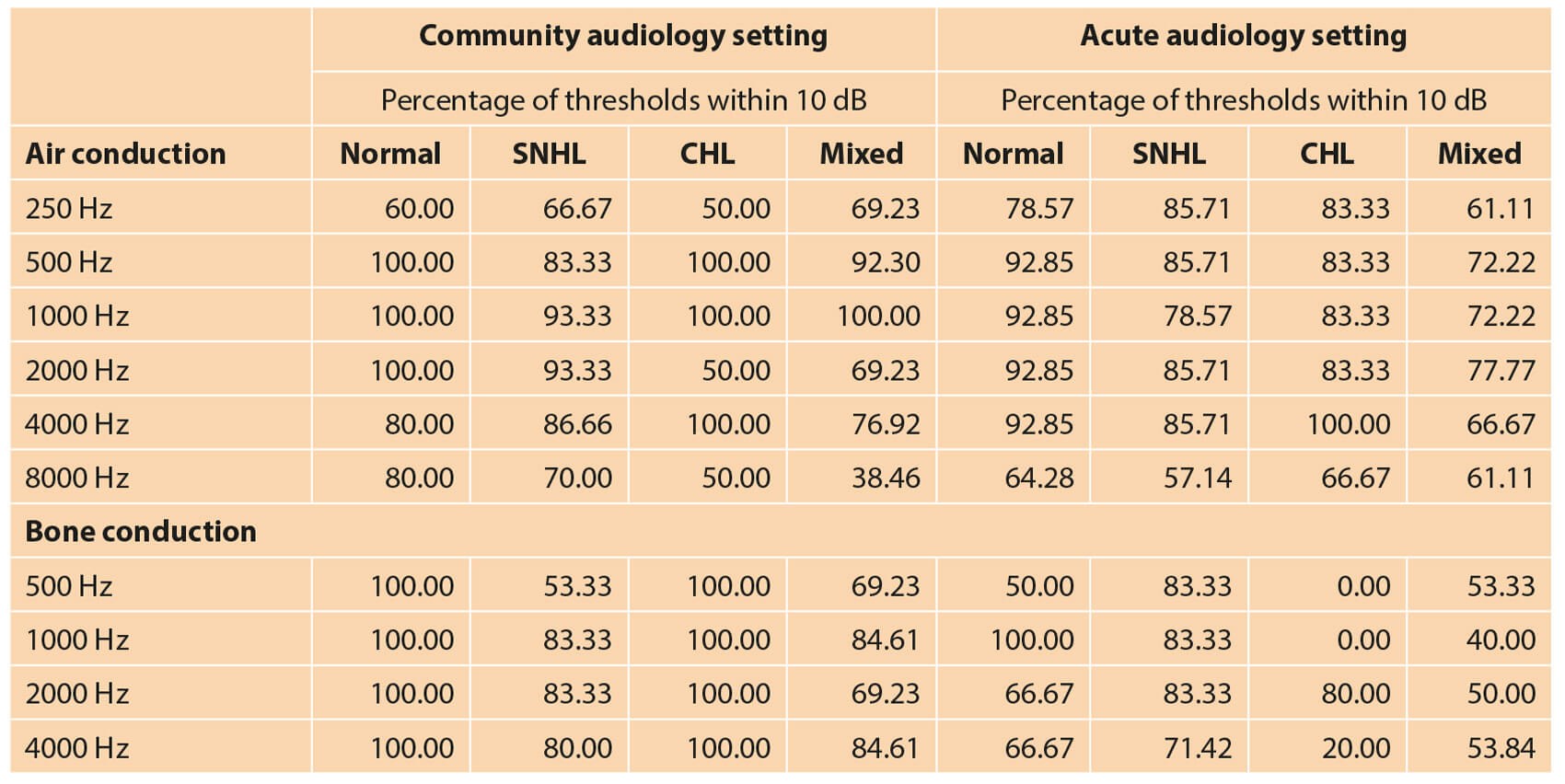
Table 3: Air-and bone-conduction threshold (including masked)
comparisons across different types of hearing loss tested via MA and AAS.
With regards to the accuracy, paired t-tests for MA-AAS thresholds were carried out across each frequency pair tested (Table 2). No significant difference was noted in the majority of frequencies of air-conduction thresholds (p>0.05). Significant differences were noted for bone-conduction thresholds especially in the acute setting (p<0.05) at 0.5, 1 and 4kHz (Table 3). The time needed to complete AAS testing was 9.09 minutes longer than the average time taken in community audiology for MA and 13.15 minutes longer than the average time taken in the acute setting. An example of the audiogram obtained via MA compared to the AAS equivalent is as shown in Figure 4.
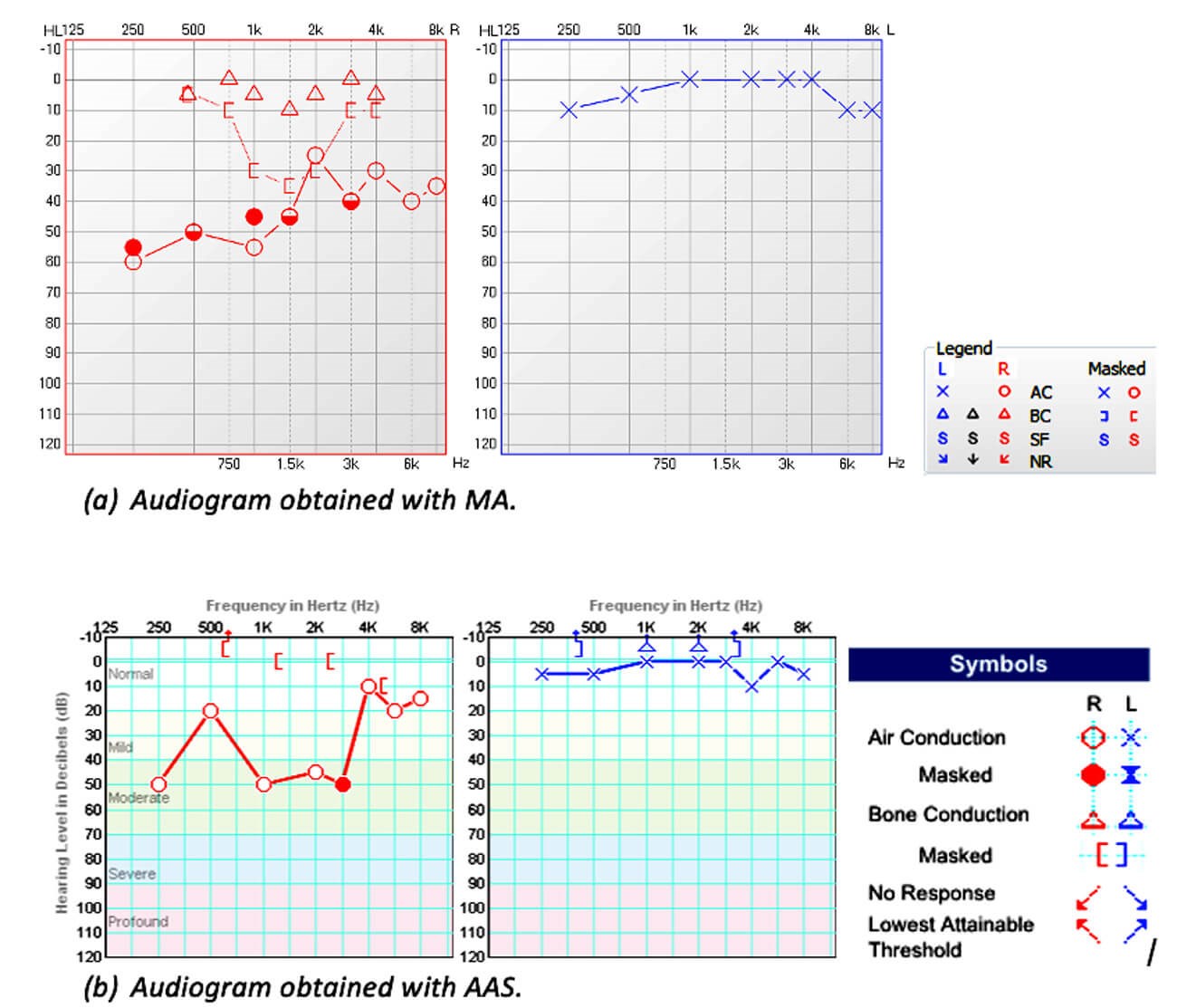
Figure 4. Example of an audiogram obtained with MA (a) and AAS (b).
Discussion
The percentage of thresholds within 10 dB was higher for air-conduction and lower for bone-conduction. This was in agreement with Yu et al (2011), who attributed the lower bone-conduction accuracy to masking challenges and forehead placement versus mastoid placement of the bone conductor [4]. Our findings revealed statistically significant differences (p<0.05) for bone-conduction thresholds between AAS and MA. This is consistent with Mahomed et al (2013), who identified nine studies in their systematic review with inconsistencies between bone-conduction thresholds using MA and AAS [5]. With regards to the shorter time needed to complete MA vs. AAS, during AAS testing, if a false or erroneous response is given, a thorough threshold-seeking procedure is followed by AAS; whereas for MA the clinician can ignore a response if the patient signifies that the response was given in error.
Conclusion
Responses obtained using AAS are comparable to those via MA in the community audiology setting but not in the acute setting. This may be because of the complexity of hearing losses in patients presenting to an acute ENT setting (conductive, mixed, unilateral losses). AAS was more time-consuming and reduced accuracy was noted in the acute setting. AAS could be beneficial in community audiology centres for routine hearing evaluations, conducted by healthcare assistants. The results will however still need to be interpreted with caution, especially in cases of conductive or mixed losses, or, where appropriate, in conjunction with other objective tests like tympanometry, acoustic reflex thresholds or otoacoustic emissions. Difficult-to-test patients would still require assessment by an audiologist. It would be beneficial to repeat this study in an acute setting with a larger population since the results obtained from AAS were significantly different for the patient cohorts seen in this setting.
References
1. British Society of Audiology (BSA). Recommended procedure: Pure-tone air-conduction and bone-conduction threshold audiometry with and without masking. 2018.
www.thebsa.org.uk/wp-content/uploads/
2018/11/OD104-32-Recommended-
Procedure-Pure-Tone-Audiometry-
August-2018-FINAL.pdf.
Last accessed April 2021.
2. Ototronix. Otogram hearing diagnostic system.
www.ototronixdiagnostics.com.
Last accessed April 2021.
3. Ho ATP, Hildreth AJ, Lindsey L. Computer-assisted audiometry versus manual audiometry. Otol Neurotol 2009;30:876-83.
4. Yu J, Ostevik A, Hodgetts B, Ho A. Automated hearing tests: applying the otogram to patients who are difficult to test. J Otolaryngol Head Neck Surg 2011;40:376-83.
5. Mahomed F, Swanepoel DW, Eikelboom RH, Soer M. Validity of automated threshold audiometry: a systematic review and meta-analysis. Ear Hear 2013;34:745-52.







