Personal protective equipment (PPE) has been a focus of attention and concern for healthcare workers around the globe during the COVID-19 pandemic. Neil Tolley discusses some of the issues.
I write this article in mid-May when, were it not for the intercession of a pandemic, I would have been enjoying a three-month sabbatical, diving in the middle of the Red Sea. In its place, I find myself, somewhat optimistically, in the midst of a pandemic and national crisis!
This has illustriously added to my personal experience of being stranded at US meetings in Denver 2001 (terrorism), Orlando 2010 (Icelandic volcano), and Boston 2012 (Hurricane Sandy). Even my tenure as YCOHNS Secretary was not without incident; the 1999 summer meeting in Disneyland, Paris, coincided with a freak cyclone, causing extensive flooding to the park and hotel, a power cut and cancellation of return flights to the UK. Entertaining wet, hungry, disappointed, and bored children was arguably my greatest challenge. Perhaps, I truly am a nautical ‘Jonah’ or a plaything of the Gods! (A ‘Jonah’ is a long-established expression among sailors, meaning a person who is bad luck.)
My damascene realisation of the impending crisis occurred on the evening of 10 March. The death and personal tragedy that has occurred to our fellow countrymen and our specialty is difficult to reconcile. Certainly, the prism through which we view life post-pandemic will be indeterminably altered.
“The irony of exchanging a Red Sea regulator for a respirator was not lost on me”
PPE has been a focus and concern for both public and healthcare workers alike. Indeed, this has rarely been out of the national consciousness. As for public health guidance, this has been inconsistent and chameleon in approach and execution. Early reports from China, Iran and Italy highlighted that otolaryngologists were at high risk due to a preponderance of AGPs (aerosol generating procedures) in their practice, the loss of our esteemed colleague, Mr Amged El-Hawrani, only adding emphasis and permeating anxiety throughout the entire ENT community.
It was apparent from an early stage of the pandemic that there would be a deluge of requests for tracheostomy, resulting in the publication of several national and subspecialty association guidelines. With tracheostomy being arguably the ‘greatest’ of all AGPs, early concerns were raised in the surgical and anaesthetic communities as to what PPE was necessary to optimise personal safety.
Enter the penultimate acronym – the PAPR or enhanced PPE. Like PPE and AGPs, if you had asked me on 10 March what they stood for, I might have failed on all three! The PAPR is an acronym for powered air purifying respirator. The irony of exchanging a Red Sea regulator for a respirator was not lost on me; I am reminded every time I donn and doff. ‘Donning and doffing’, yet more C19 lingua franca.
The essential composition of a PAPR is a battery-powered fan which extracts air from the environment, passes it through a HEPA filter (high efficiency particulate air) and, via a hose, delivers the filtered air to an immersive surgical hood. Both the hood and HEPA filter are the essential components. Due to the significant range of PAPRs on the market of variable quality and price, it is an absolute requirement that the safety standards of the device and filter be verified before committing to a purchase. Your safety may depend upon it, and I strongly advise that you do not leave this to the vagaries and whims of the hospital procurement system to make a choice on your behalf – be involved!
As well as providing enhanced protection, the PAPR has the advantage of mitigating fit testing. Don and doff training is, nonetheless, an essential perquisite for its proper use. PAPR can provide a nominal protection factor 10 times greater than a standard FFP3 mask; the latter with eye protection stands as national PHE guidance from 2 April 2020. Politically, this makes it difficult for healthcare workers to persuade their hospital to procure PAPR as this contravenes national guidance and this is where your challenge will reside. Nonetheless, this is far from insurmountable.
FFP3/N95 masks are not intended to be used for operations taking longer than an hour, as stipulated by health and safety executive law (HSG53 Fourth Edition 5/2013). There is no single mask that fits every facial geometry. It is also an issue for those who cannot shave facial hair for religious or cultural reasons; they are both uncomfortable and their fit efficiency is inconsistent during prolonged use. Guidance from the health and safety executive recommends powered hoods for procedures taking longer than an hour. Conveniently for healthcare workers, this guidance has gone unnoticed by PHE. You therefore have the law on your side, which heralds a welcome change for the surgical community!
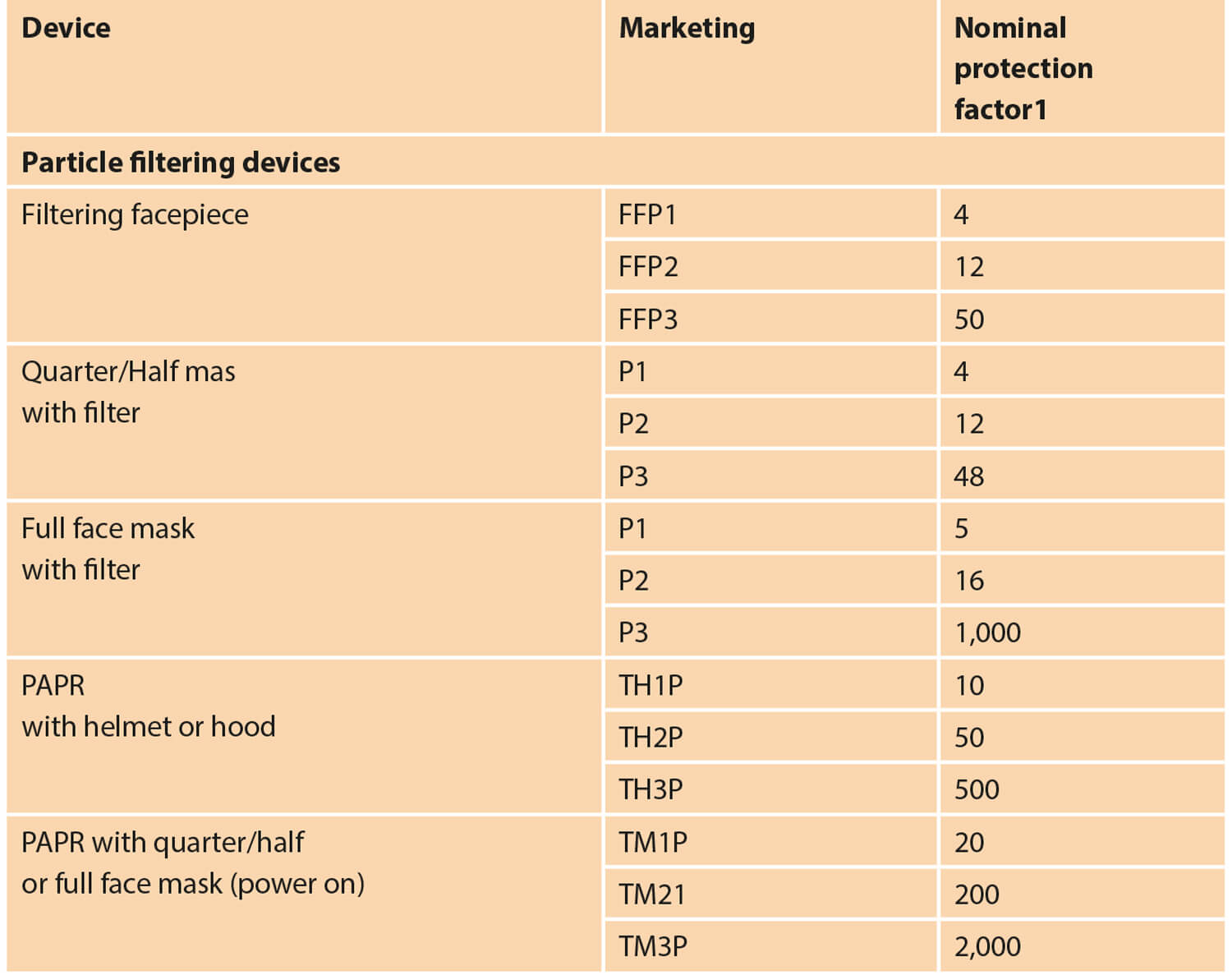
Figure 1.
A summary of comparative protective values for PPE is shown in Figure 1. These do not factor in those attributable to the HEPA filer which, in the Tecmen P3, has a capture efficiency of 99.97% and a penetration level of <0.03%. This compares to efficiency and penetration levels of >95% <5% for the N95. The Coronavirus is very small at 140nm, and an effective HEPA filter is fundamental to the safety of the PAPR.
“PAPR can provide a nominal protection factor 10 times greater than a standard FFP3 mask”
At Imperial, we were able to procure the Tecmen P3 HEPA filter (EN12941 PRSL) imparting a capture efficiency of >99.996%. This has allowed a return to managing emergencies in standard fashion, permitted skull base, head and neck and airway surgery, and has assisted with the considerable tracheostomy workload – it has been an absolute game changer!
Tecmen PAPRs can be sourced from a single UK supplier (weldfastuk.co.uk/). I declare no conflict of interest, only the safety of colleagues.


