Should patients take charge of their own cochlear implant care? Helen Cullington presents a compelling case that will provoke discussion in implant centres.
Around 1400 people receive a cochlear implant in the UK each year. Patients require lifetime annual follow-up [1] at one of 18 specialist centres, which may be several hours away from their home.
All essential National Health Service (NHS) cochlear implant care is provided free of charge at the point of delivery. However, there are other costs associated with attending appointments, e.g. travel costs, lost income, childcare, accommodation and parking. Some deaf people may not feel confident to travel by public transport alone, so there may be additional costs for an accompanying person. In addition to financial costs, there are also time constraints, social inconvenience and psychological barriers associated with a journey to hospital. For patients attending our Southampton centre, the average travel distance is 46 miles, suggesting that the average driving cost of a round-trip journey to the centre is more than £40.
“We should be in control as much as possible of our own hearing destiny.”
What happens now?
Currently the cochlear implant centre provides lifelong care, following a schedule of appointments with little opportunity for personalisation; this may result in appointments occurring which do not provide benefit. Conversely, when some patients attend a routine appointment, an audiologist can diagnose that there has been hearing deterioration which the patient had not noticed. This is often remedied by replacing equipment that the patient could have done at home. Empowering the patient to self-care at home would enable more stable hearing and a more convenient and accessible service.
Why would we want to put patients in charge of their own care? Surely we are the experts?
In the UK, we have all grown up with the traditional NHS “doctor knows best” attitude. Let’s turn that on its head: in fact patients are the experts in their condition, lifestyle and individual needs. People with long-term conditions drew the picture in Figure 1 to show what it is like for them.
Figure 1. Representation of living with a long-term condition, drawn on a paper tablecloth by a person with a long-term condition (reproduced with kind permission of Year of Care Partnerships, http://www.yearofcare.co.uk/).
Assuming that a person with a cochlear implant currently has three hours per year of clinician interaction (annual follow up appointment, repairs, support phone calls etc.), this means that the patient is already self-caring 99.9% of the time! We need to move towards a care model that acknowledges and supports this.
There is much evidence to show that people who are activated and empowered – possessing the knowledge, skills and confidence to manage their condition effectively – have better health outcomes and care experiences [2]. Clinicians are often concerned that patients with lower empowerment, poor health literacy and difficult social circumstances will struggle to self-care; in fact they have the most to gain [2]. There are many barriers to introducing this (or indeed any) change; our work with stakeholders has identified some key driving and resisting forces, as shown in Figure 2.
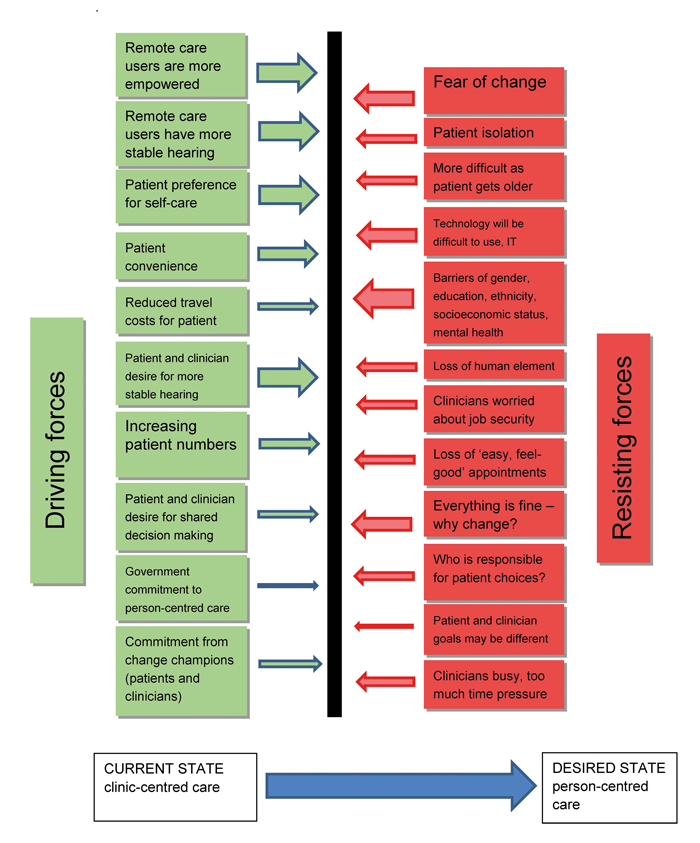
Figure 2. Driving and resisting forces to consider when making a change to person-centred care. Some potential benefits of person-centred cochlear implant care.
At the University of Southampton Auditory Implant Service, we are working to make the cochlear implant care pathway person-centred and provide a more efficient service to allow quicker identification of problems. We designed, implemented and evaluated a long-term follow-up pathway for people with cochlear implants, offering them remote self-monitoring, self-adjustment of devices, and a personalised online intervention package for testing their own hearing and accessing rehabilitation, troubleshooting and training at home [3].
“We love seeing you at the cochlear implant centre… but lets put you in charge of deciding when you want to come.”
We ran a six month clinical trial with 60 people randomised to either the remote care pathway or a control group who followed their usual appointment schedule. The main outcome evaluated was empowerment. We found that only the remote care group had a significant increase in their cochlear implant empowerment after using the remote care tools. Quality of life remained stable in the two groups. The hearing test result in clinic had improved in the remote care group, although they had not noticed a change. The control group, however, felt their hearing had become slightly worse. This may suggest that the remote care group were more able to take action to keep their hearing stable during the trial.
Patients and clinicians were generally keen to continue remote care, with the most popular aspect being the home hearing test (http://bit.do/remote_care).
We would like to spread these benefits to many more people using cochlear implants. We believe that using a remote care person-centred model instead of the usual clinic-centred model will provide better long-term outcomes to people with cochlear implants: higher empowerment, and more stable hearing. We would like to move to a model where patients, clinicians and families decide together when an appointment is needed, rather than the clinic-centred routine appointment schedule.

Putting patients in charge of their own care.
Clinician knows best? No way. Let’s work together with patients and their families to empower and support them to take charge of their own care. Please get in touch to find out more.
References
1. British Cochlear Implant Group. Quality Standards. Cochlear implant services for children and adults. 2016; https://www.nuh.nhs.uk/media/2318993/
bcig-quality-standard-2016.pdf
2. Hibbard JH, Greene J. What the evidence shows about patient activation: better health outcomes and care experiences; fewer data on costs. Health Affairs 2013;32(2):207-14.
3. Cullington HE, Kitterick P, DeBold L, et al. Personalised long-term follow-up of cochlear implant patients using remote care, compared with those on the standard care pathway: study protocol for a feasibility randomised controlled trial. BMJ Open 2016;6(5):e011342.
Declaration of competing interests: None declared.


