Middle ear cleft cholesteatoma is an inflammatory disease that erodes local bony structures and can cause otorrhea, hearing loss, vertigo and intracranial complications. It is usually treated with surgery, typically canal wall up (CWU) or canal wall down (CWD) surgery. CWU surgery has the benefit of restoring hearing conduction, allowing comfortable fitting with a hearing aid and less postoperative aural toilet.
It is, however, associated with a higher rate of residual and recurrent disease than CWD surgery and a mandatory ‘second look’ revision procedure is performed after nine to twelve months. Imaging allows a non-invasive alternative in detecting recurrent and residual cholesteatoma following CWU surgery and non-echoplanar diffusion weighted magnetic resonance imaging (DWI) is currently the imaging modality of choice to do this [1-3].
DWI is a quick MRI examination sequence which takes about 15 minutes to perform. It can be performed on a standard 1.5T MRI scanner but may require a software upgrade to do this. It does not involve radiation or require administration of intravenous contrast medium. For imaging middle ear cholesteatoma, the non-echoplanar type of DWI [such as HASTE (Half-Fourier Acquisition Single-shot Turbo Spin Echo) or PROPELLER (Periodically Rotated Overlapping ParallEL Lines with Enhanced Reconstruction) sequence] is preferred to the echoplanar type (used in brain imaging and neck cancer imaging) as it has a finer imaging matrix and lacks the air-bone interface artefacts that can impair the diagnostic performance [1, 2]. For the detection of postoperative middle ear cholesteatoma, the MRI examination is typically performed at our institution by acquiring 2mm thick coronal T2-weighted images to delineate the anatomy of the middle ear cleft and copy-referencing them with the 2mm thick coronal non-echoplanar HASTE sequence images acquired with b-values of 0 and 1000 s/mm2 to detect the cholesteatoma [4].
The apparent diffusion coefficent (ADC) map is also reconstructed after the scan using the diffusion scan raw data and this allows the ADC value of the lesion to be calculated [4]. Cholesteatoma, by virtue of its keratin content, produces high signal intensity on DWI obtained with b-values of 800 or 1000 s/mm2 (Figure 1) and corresponding low signal on the ADC map. The high signal of cholesteatoma on diffusion weighted images is a result of restricted molecular diffusion but also due to a ‘T2 shine through effect’ that occurs in tissues with high T2 signal intensity and ADC values less than brain [1, 2]. The ADC values of postoperative middle ear cleft cholesteatoma have been shown to be significantly lower than that of non-cholesteatomatous tissue [4].
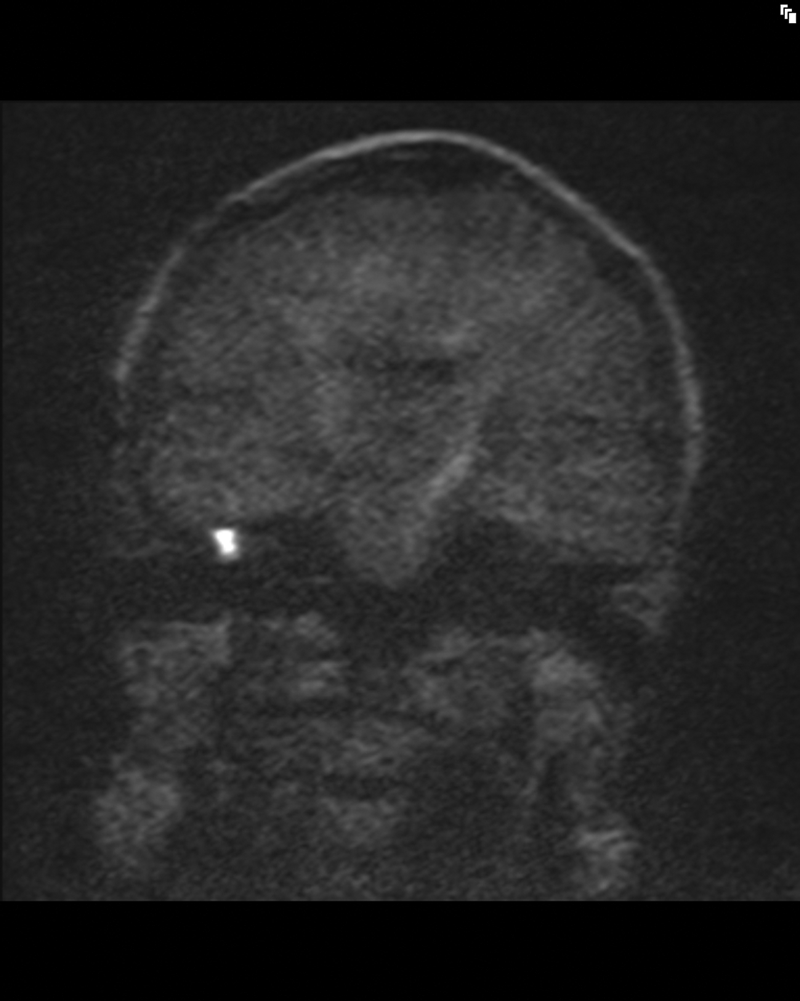
Figure 1: Coronal HASTE diffusion weighted b1000 image shows high
signal cholesteatoma at post-operative right middle ear cleft.
Non-echoplanar DWI (such as HASTE or PROPELLER sequence) has the ability to detect cholesteatoma as small as 2mm, with many studies reporting a sensitivity and specificity between 90-100% in the detection of cholesteatoma [1-5]. It performs better than its echoplanar counterpart as it has a higher spatial resolution without air-bone interface artefact [1, 2]. The main limitation of DWI is its lack of sensitivity to reliably detect an evacuated cholesteatoma sac or small keratin pearls less than 2-3mm in size. False positive findings are less of an issue and include bone powder, silastic sheets, cholesterol granulomas and cerumen in the ear canal. Quantitative detection of cholesteatoma with ADC values also has good accuracy for detecting cholesteatoma and can supplement the qualitative method of detecting cholesteatoma [4]. The diagnostic performance of non-echoplanar DWI is also superior to that of CT and delayed post-contrast MRI [1, 2, 6].
In addition to detecting postoperative cholesteatoma, non-echoplanar DWI HASTE sequence performs well in predicting the location of cholesteatoma [7]. Unlike the DWI PROPELLER sequence, the HASTE sequence allows acquisition in the coronal plane which is especially useful for localising disease [1, 2, 7]. DWI may underestimate the true size of cholesteatoma [7]. With information provided by DWI on the presence, location and size of the residual or recurrent cholesteatoma, the surgeon can confidently provide a more accurate and detailed consenting process with the patient able to ‘see’ their disease and be better informed. The surgeon can also plan the most appropriate approach and possibly better utilise theatre time.
Given the compelling evidence from the many small studies supporting its good diagnostic performance in detecting postoperative cholesteatoma, non-echoplanar DWI has been proposed for screening postoperative cholesteatomas, thus obviating many ‘second look’ surgical procedures [1, 2, 5]. Avoiding surgery would have financial benefits and reduce potential surgical morbidity. However, a negative DWI scan cannot exclude a small residual or recurrent cholesteatoma and screening with DWI would require serial scanning over a period of time prior to discharge. Further studies are required to evaluate the duration of follow-up, cost-effectiveness and risk of not carrying out ‘second look’ procedures. The main practical drawback would be the risk of a patient with residual cholesteatoma becoming lost in the follow-up pathway.
References
1. Mas-Estelles F, Mateos-Fernandez M, Carrascosa-Bisquet B, et al. Contemporary non-echoplanar diffusion-weighted imaging of middle ear cholesteatomas. Radiographics 2012;32:1197-213.
2. Khemani S, Singh A, Lingam RK, Kalan A. Imaging of postoperative middle ear cholesteatoma. Clin Radiol 2011;66:760-7.
3. Li PM, Linos E, Gurgel RK, et al. Evaluating the utility of non-echo-planar diffusion-weighted imaging in the preoperative evaluation of cholesteatoma: a meta-analysis. Laryngoscope 2013;123:1247-50.
4. Lingam RK, Khatri P, Hughes J, Singh A. Apparent diffusion coefficients for detection of postoperative Middle ear cholesteatoma on non-echo-planar diffusion weighted images. Radiology 2013;269:504-10.
5. Huins CT, Singh A, Lingam RK, Kalan A. Detecting cholesteatoma with non-echo-planar (HASTE) diffusion-weighted magnetic resonance imaging. Otolaryngology Head Neck Surgery 2010;143:141-6.
6. De Foer B, Vercruysse JP, Bernaerts A, et al. Middle ear cholesteatoma: non-echo-planar diffusion-weighted MR imaging versus delayed gadolinium-enhanced T1-weighted MR imaging—value in detection. Radiology 2010;255:866-72.
7. Khemani S, Lingam RK, Kalan A, Singh A. The value of non-echo-planar HASTE diffusion-weighted MR imaging in the detection, localisation and prediction of extent of postoperative cholesteatoma. Clin Otolaryngol 2011;36:306-12.
Declaration of Competing Interests: None declared.



