Professor Ahmed Geneid is a laryngologist and phoniatrician at Helsinki University Hospital and a founding member of the International Association of TransVoice Surgeons. Here, he presents the intricacies and nuances of gender-affirming voice surgery after own hospital’s 30 years of experience in this field.
Voice and transgender
Gender identity and its perception and acceptance in different societies have gone through major transformations in recent decades. Historically, different accounts confirm the presence of transgenderism in ancient civilisations, ranging from ancient Egypt, Greece and Rome to different indigenous tribes in the Indian subcontinent.
Although the term ‘transgender’ only emerged in the 1950s and 1960s, it describes a reality that preceded such terminology by thousands of years. Gender identity is greatly influenced by how voice is perceived by others. As such, the voice plays a crucial role in expressing one’s gender and self-image.
In the Western world, the ratio of male-to-female transgenders is approximately 3:1. Phonosurgery for trans women is mainly offered to align their voices with their gender identity. Such desire is not only to increase the voice pitch to achieve the female range of fundamental frequency (F0) but also to acquire, if desired, a feminine type of communication. In most clinical practices, it is common to start with offering trans women the assistance of voice therapy. However, many still feel dissatisfied with their voices, particularly when it unexpectedly reverts to a male-sounding tone during uncontrolled situations, such as yawning, laughing, coughing, or shouting. In addition to trans women, and in relatively rare cases, even biologically born females may require pitch-raising surgery due to a naturally low F0 of their voice.
Phonosurgery for raising voice pitch
Four main surgical techniques have been developed to raise voice pitch. One previously popular technique introduced by Isshiki in 1983 is cricothyroid approximation [1]. This approach attempts to increase tension in the vocal folds and raise the F0. However, cricothyroid approximation is no longer preferred due to risk of suture tearing and because it results in an unnaturally tense voice with diminished intonation and only temporary voice improvement.
"Although the term ‘transgender’ only emerged in the 1950s and 1960s, it describes a reality that preceded such terminology by thousands of years"
A second technique proposed by Wendler in 1990 has gained tremendous popularity in recent decades [2]. In Wendler’s glottoplasty, suturing the anterior part of the vocal folds together results in shortening of their functional length and marked increase in the F0 of the patient’s voice. A third technique by Orloff in 2006 suggested a different approach involving a lateral cordotomy incision using CO2 laser, which increases the stiffness of the vocal folds and results in an increase of F0. Such technique is refered to as Laser-Assisted Voice Adjustment (LAVA) [3].
The last and fourth technique, proposed by Thomas in 2013, is called feminisation laryngoplasty [4]. This technique aims to increase the F0 and modify the vocal tract. This method is performed via laryngofissure and involves resecting segments of the thyroid lamina and true and false vocal folds. This creates a new anterior commissure and reduces the length of vocal fold. It additionally entails thyrohyoid elevation.
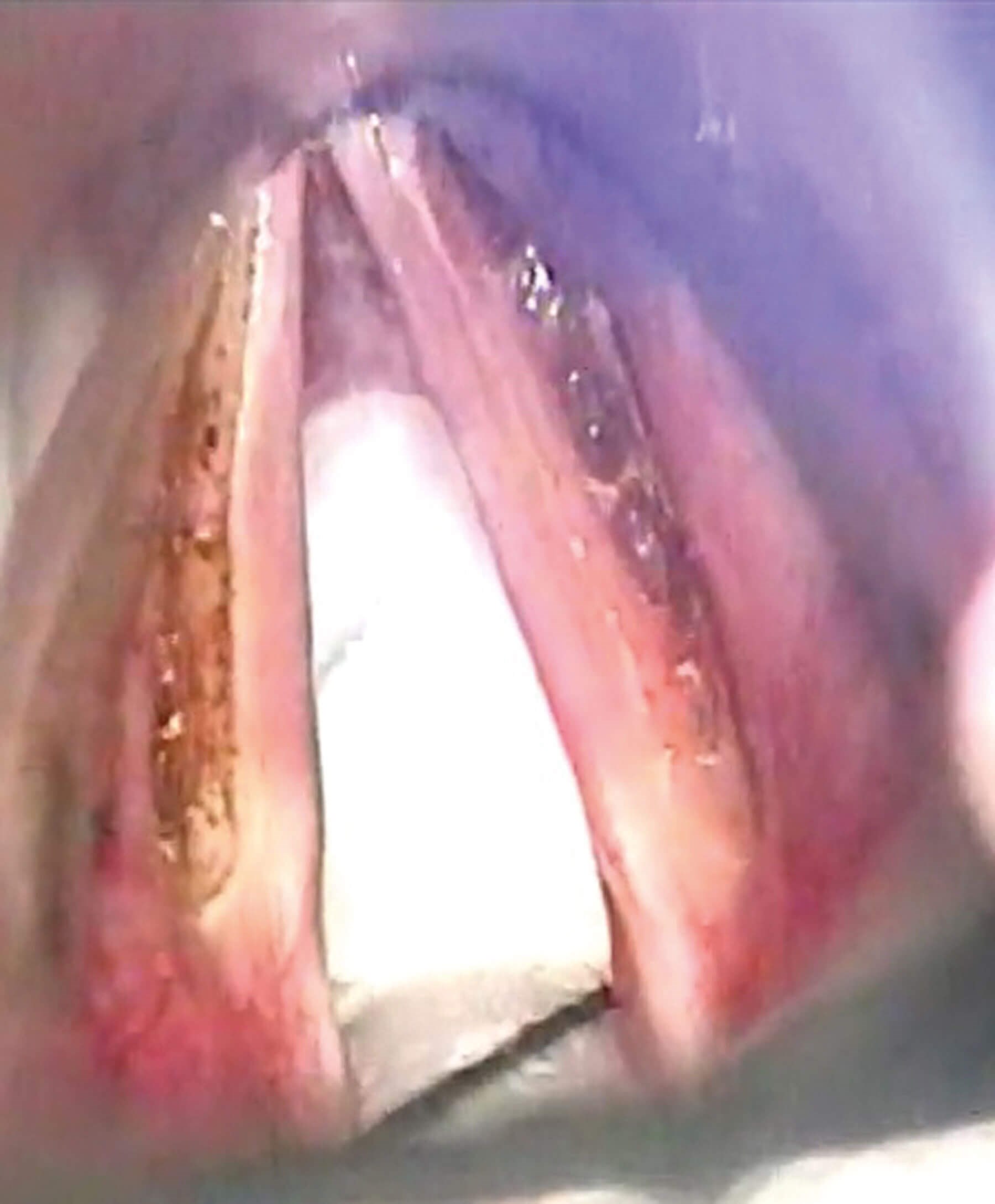
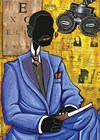
Figure 1. Intraoperative picture of deep LAVA on both vocal folds.
Determining the most effective surgical method has been a subject of ongoing exploration. However, it is clear from current clinical practice and literature that Wendler glottoplasty is becoming the mainstay and best practice for transgender females. Feminisation laryngoplasty with laryngofissure requires further evaluation, particularly regarding benefits related to vocal tract changes and possible complications.
How to raise the pitch - surgical techniques for Wendler glottoplasty and laser reduction of the vocal fold mass
Human male vocal folds vibrate at approximately 100 times per second, resulting in an acoustic pitch of approximately 100 Hz. Women, on the other hand, have twice the number of vibrations, with vocal folds vibrating at approximately 200 times per second. The F0 of women’s voices is, thus, approximately 200 Hz.
"Cricothyroid approximation is no longer preferred due to risk of suture tearing and because it results in an unnaturally tense voice with diminished intonation and only temporary voice improvement"
In current practice, the laryngologist can choose between laser reduction of the vocal fold mass by deep LAVA-like laser incision, glottoplasty, or a combination of both. The choice is mainly based on the patient’s requests and expectations from surgery. Applying a deeper version of LAVA, in which a lateral incision is performed with a CO2 laser (or blue laser under local anaesthesia) will result in a reduced mass of the vocal fold and an almost invisible scar later to the free edge of the vocal fold. This will usually result in a 10-20 Hz increase in F0 of the patient. Such an increase is usually sufficient for a biological woman with a socially disruptive gender-neutral voice. It may also be sufficient for a transwoman with gender-neutral voice.
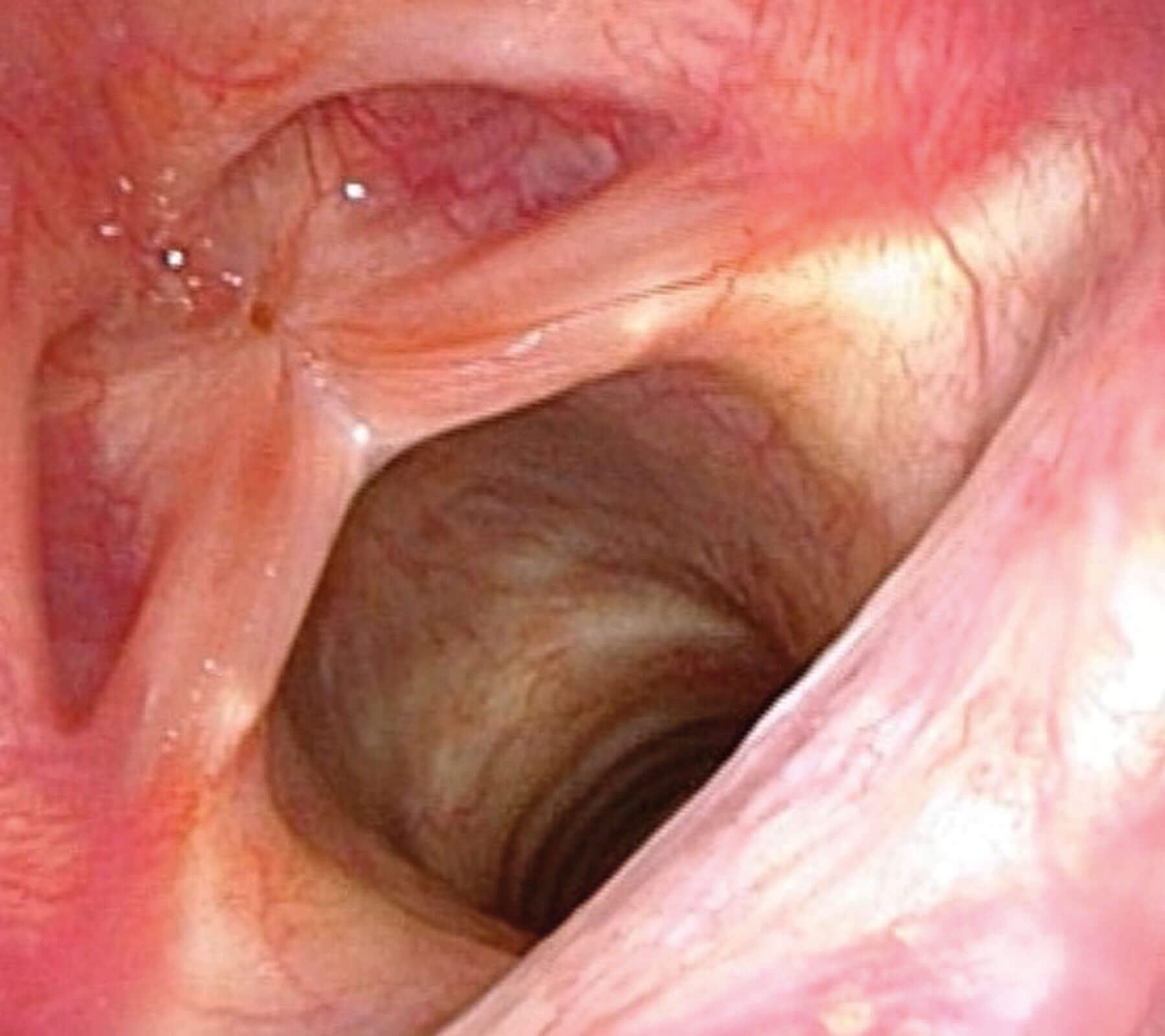
Figure 2. Postoperative picture of glottoplasty web five months after operation.
Figure 3. Same patient as in Figure 2 during end of open-phase of glottal wave.
On the other hand, if there is a need to increase the voice F0 by about 50-100 Hz, then a combination of Wendler glottoplasty and deeper LAVA is preferred [5]. In this surgical approach, approximately 40-50% of the vibrating edge of the vocal folds is de-epithelised using CO2 laser or cold instruments. These parts are to be sutured together with non-absorbable or absorbable sutures depending on surgeon preference. Absorbable thread can cut through, while non-absorbable thread can result in a granuloma above the thread that will disappear spontaneously within six to eight months. The goal of suturing is to bring the anterior parts of the vocal folds together, which thus reduces the vibrating portion of the vocal folds to 50-60% of its previous length. Additionally, laser reduction of the vocal fold mass by lateral incisions will also reduce tension at the suture site. Finally, tissue glue is applied over the sutures to ensure their durability and integrity. A three-minute video of the author’s technique is available on YouTube – https://www.youtube.com/watch?v=k4cskwpjlz4.
"It is clear from current clinical practice and literature that Wendler glottoplasty is becoming the mainstay and best practice for transgender females"
It is worth mentioning that different modifications of Wendler glottoplasty are practised. These include, but are not limited to, suturing the de-epithelised anterior parts of the vocal folds together with sutures going through subglottis to increase tension while drawing anterior commissure caudally. Some also prefer to inject Botox into the vocal folds in conjunction with the operation. Another modification joins both endoscopic and open approaches in passing the thread from outside the larynx into both vocal folds.
Phonosurgery to lowering the voice pitch
A minority of female-to-male transgenders may require lowering of the voice F0. This is typically achieved through androgen administration and is relatively unproblematic. If such hormonal treatment is not possible or does not result in the desired effect, a type 3 thyroplasty aiming to reduce the tension of the vocal folds from inside is a suitable approach. The procedure is performed under local anaesthesia by removing a vertical part of the thyroid lamina approximately five to seven millimetres from midline or by pushing the anterior commissure backwards.
Summary
Voice plays a large role in gender perception, and therefore phonosurgery is an important part of trans healthcare. This is particularly the case for trans women, where there are different techniques which may be modified and combined to raise the FO of the voice. In terms of trans women, Wendler glottoplasty is emerging as the most preferred option.
References
1. Isshiki N, Taira T, Tanabe M. Surgical alteration of the vocal pitch. Journal Otolaryngol 1983;12(5):335-40.
2. Wendler J. Vocal pitch elevation after transsexualism male to female. Proceedings of the Union of the European Phoniatricians; Salsomaggiore, Italy, 1990.
3. nOrloff LA, Mann AP, Damrose JF, Goldman SN. Laser‐assisted voice adjustment (LAVA) in transsexuals. The Laryngoscope 2006;116(4):655-60.
4. Thomas JP, MacMillan C. Feminization laryngoplasty: assessment of surgical pitch elevation. Eur Arch Otorhinolaryngol 2013;270:2695-700.
5. Geneid A, Rihkanen H, Kinnari TJ. Long-term outcome of endoscopic shortening and stiffening of the vocal folds to raise the pitch. Eur Arch Otorhinolaryngol 2015;272:3751-56.