en·tre·pre·neur, noun a person who organises and operates a business and who has qualities of leadership, initiative and innovation.
In the United States, facial plastic surgery (FPS) services are divided among private and academic practices. The vast majority of academic surgeons are not allowed to operate their own private offices (nor do they typically have the time to do so). Aesthetic surgery is paid out-of-pocket by the consumer and is therefore more profitable than procedures covered by health insurance plans. Whereas a collaborative relationship exists between university FPS surgeons and the community for reconstructive patients, there is competition for the more limited cosmetic patients.
Numerous studies support facial plastic surgery as a profitable enterprise at a university [1, 2]. Creating a successful FPS practice within the confines of a university system requires making the most of advantages and limiting the disadvantages of an academic position. One major advantage of an academic surgery appointment is our position as experts within the community. This can be promoted via interaction with a university public relations department and local media outlets. Academic physicians also have greater opportunities to perform translational research with local private enterprise. Of course, there is also the advantage of greater financial stability through cost and profit sharing within the university. This includes shared support departments, such as information technology and biomedical engineering that help maintain computer systems and equipment.
There are also many disadvantages inherent to an academic FPS practice. In the USA, decreasing insurance reimbursement, decreasing governmental support, a highly competitive private sector and the unknowns of the Affordable Care Act have led hospital administrators to be more conservative with resources than they were 20 years ago[3, 4]. There are high fixed costs of operating at university hospitals, which necessitates lowering the academic physician’s portion of a cosmetic fee to remain competitive with community prices. High operational costs and decreasing profits lead to an overriding theme of communal space in the decision-making mindset of the university administration. In turn, this leads to a perception in the community, real or imagined, of non-personalised delivery of care. Complicated automated phone systems, large facilities, difficult parking and variable staff encounters contribute to an unwelcoming experience. Although sharing support staff and clinic space maximises utilisation, it is observed as impersonal to the consumer.
Academic practice models
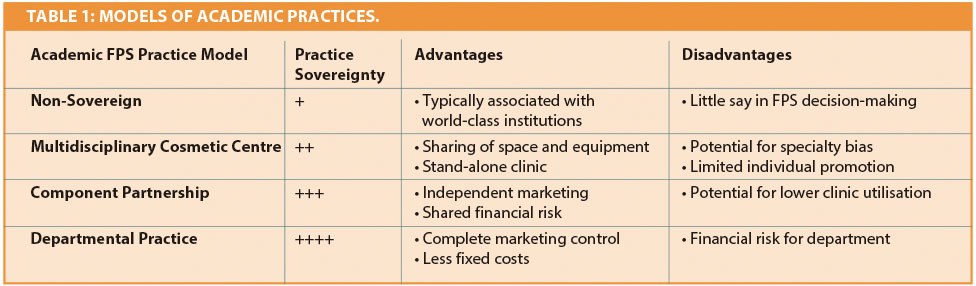
Entrepreneurial opportunities depend greatly on the facial plastic surgery practice model that exists at the institution. Practice models may be categorised by the degree of practice sovereignty that exists from the facial plastic surgeon’s perspective (Table 1). The ‘non-sovereign’ practice is exemplified be many of the USA’s top private ‘clinic’ hospital systems. Though world-renowned medical institutions, there is no marketing of individuals or individual practices. Resources are shared between departments and administrators generally make practice decisions. New patients typically present to the clinic because of the excellent reputation of the institution, not necessarily because of the individual practitioners. Next on this continuum is the academic ‘Multidisciplinary Cosmetic Center’, which brings academic physicians from different departments together under a single roof. This has the advantage of better clinic utilisation and facilitates the sharing of equipment and other resources [5]. However, there is a potential for specialty favouritism and individual specialties may not be able to run promotions for procedures where specialty overlap exists.
The ‘Component Partnership’ model allows a department to independently brand a FPS practice under the umbrella of the university and market it separately. An example of this is the Visage Center at the University of Colorado (www.VisageCenter.com), which provides FPS services for the University of Colorado. While the department makes many of the practice decisions, a close partnership with the university is maintained. Unless there are sufficient surgeons on staff, this model may lead to suboptimal clinic utilisation, which can make it difficult to obtain funding for stand-alone offices, new equipment, etc. Finally, in the ‘Departmental Practice’ model the otolaryngology department acquires a loan to build and equip a FPS practice, giving complete control of the practice to the department. However, the department also accepts all of the financial risk and must develop systems to manage a clinic.
“Creating a successful cosmetic facial plastic surgery practice within the confines of a university system requires making the most of advantages and limiting the disadvantages of an academic position.”
Creating a team
Economist Robert Reich considers team-building, leadership and management ability essential qualities for the entrepreneur. Whichever model exists at the institution, there are certain challenges that must be met. Assembling an excellent cosmetic practice team is one such challenge. In the spirit of sharing resources, nurses and medical assistants in a university setting often ‘float’ between providers and clinic locations. This creates difficulty in training staff and creates a culture of non-responsibility and non-ownership in the success of the practice. This is in stark contrast to the small private office, where the success of the practice correlates directly to their employment. Patients readily detect this fundamental difference. Furthermore, physician extenders at an academic institution are often called upon to be financially self-sufficient. The revenue generated by an aesthetician, for example, must cover salary and benefits, which is difficult if downstream revenue is not considered. Regardless, these challenges must be met since without these team members, a successful cosmetic FPS practice is exceptionally difficult to obtain.
Marketing and social media
If individual practice promotion is permitted, marketing, website development and social media (Facebook, Pinterest, Twitter, YouTube) are areas where entrepreneurship may be exercised. To compete with the private sector, the academic FPS website is ideally built and maintained separate from the university website. This alleviates the need for cosmetic patients to navigate through a multitude of hospital web pages or to use an often-imperfect site search box. Such an arrangement also allows for search engine optimisation, which can independently push the practice website higher on web searches. Practice-specific social media also provides unique branding opportunities. While word-of-mouth, a well designed website and physician referrals are still the main source of new patients [6, 7], the impact of social media sites is growing [8]. They provide an opportunity to quickly distribute practice information and promotions to the community. In addition, creating practice ‘friends’ improves brand loyalty and is a means of bringing new patients to the university hospital system at large.
New products
New products come onto the market with great frequency and are marketed directly to the consumer. Patients often present to the office asking for the latest filler, technology or treatment by name. In the case of new medications, this can be problematic. For example, over the last two years, several neuromodulators have come onto the market to compete with Botox Cosmetic® (Allergan Inc, Irvine, CA). However, duplicate medications are not permitted on hospital pharmacy formularies. Appropriately, it is the mission of a university to base decisions on evidence, and obtaining approval for new medications requires demonstration of superiority over existing options. To offer new products to the consumer, therefore, the academic surgeon must initiate this process with the university pharmacy department and provide evidence to support those products. These activities minimise the risk of offering ‘snake oil’ to the consumer and further establish the university as trustworthy in the community. Summary Cosmetic facial plastic surgery at a university institution presents unique challenges. However, in the USA, if one is to compete with community surgeons, the academic FPS practice must be approached as if it were a private enterprise. This requires constant communication and a great deal of ‘asking’ from the university administration. In the end, navigating these issues depends on the academic surgeon’s ability to interact with university administration and on the reciprocal understanding of the needs of a cosmetic FPS practice. If an understanding may be reached, the many advantages of an academic FPS practice may be realised.
References
1. Alsarraf R, Larrabee WF, Jr, Johnson CM, Jr. Cost outcomes of facial plastic surgery: regional and temporal trends. Arch Facial Plast Surg 2001;3(1):
44-7.
2. Pacella SJ, Comstock MC, Kuzon, WM, Jr. Facility cost analysis in outpatient plastic surgery: implications for the academic health center. Plast Reconstr Surg 2008;121(4):1479-88.
3. Ruberg RL. Can academic plastic surgery survive? Ann Plast Surg 2004;52(3):329-30.
4. Chandawarkar RY, Dutta S. Dynamics of hospital-based plastic surgery. Plast Reconstr Surg 2007;119(2):730-7.
5. Rao VK, Schmid DB, Hanson SE, et al. Establishing a multidisciplinary academic cosmetic center. Plast Reconstr Surg 2011;128(6):741e-6e.
6. Adamson PA, Zavod MB. Changing perceptions of beauty: a surgeon’s perspective. Facial Plast Surg 2006;22(3):188-93.
7. Nowak LI, Washburn JH. Patient sources of information and decision factors in selecting cosmetic surgeons. Health Mark Q 1998;15(4):45-54.
8. Vardanian AJ, Kusnezov N, Im DD, et al. Social media use and impact on plastic surgery practice. Plast Reconstr Surg 2013;131(5):1184-93.
Declaration of Competing Interests: None declared.


