The traditional adenoid curette more closely resembles a medieval torture device than an instrument of cure. Therefore it is not much of a surprise to learn that it has changed little since its invention almost 150 years ago. During that time, ENT surgery has been revolutionised by microscopes, endoscopes and lasers - so why has the adenoidectomy been left behind?
Wilhelm Meyer, an ostracised Danish otolaryngologist, first published his treatise on curetting “adenoid vegetations” in 1870, noting its success in improving deafness, hypernasal speech and “vacant and stupid countenances” in his patients [1]. Popularity for his technique snowballed as it was touted as a cure for everything from anorexia, “mental retardation”, bad dreams and masturbation. By 1900, Sir Felix Semon was unveiling a statue of Meyer in Copenhagen [2]. In 1906 the New York education authority was so enthusiastic about this method to boost academic performance, it sanctioned mass adenoidectomies on school children (without parents’ consent or even knowledge) - prompting the ‘Adenoid Riots’ in Brooklyn [3].
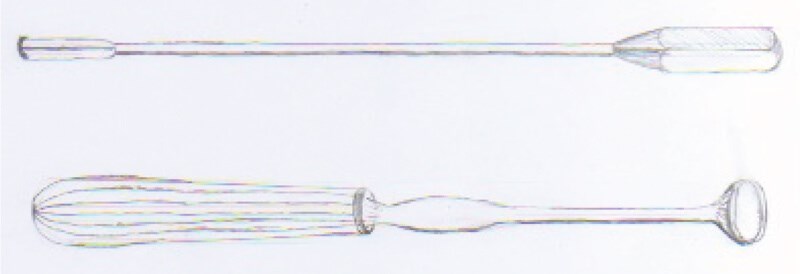
Figure 1. Illustration of Nasopharyngeal Radium Applicator (top) and Meyer’s Adenoid Curette (bottom).
When the US entered World War Two, it was found that a large proportion of pilots and submariners were being grounded by “aerotitis media”, believed to be caused by large adenoids. The armed forces could not afford time for their men to recuperate from a surgical adenoidectomy and turned to radium for a solution. Radium was in vogue in the US; discovered by the Curies in 1898 it was now utilised in everything from watch dials to toys and spas. In this instance, radium-tipped rods were inserted into the post nasal space to shrink the adenoids, improving Eustachian function. Servicemen were exposed to 2000 rads, for eight to 12 minutes, several times across two weeks (by contrast an X-ray is 0.1 rad). Contemporary studies declared this method a success, and it is estimated that up to 2.5 million children and servicemen were eventually treated, until the 1960s. It was also a popular procedure in the Netherlands.
By the 1990s, a growing appreciation of the side-effects of radium led to calls to evaluate the long-term health of those who had received nasopharyngeal radium.
However, this has proven difficult. Several studies have shown an increased incidence of head and neck cancer but this was statistically insignificant. Kang et al showed an increased risk of circulatory disease and increased risk of mortality for all causes (OR 1.32, 95%CI 1.14-1.53) in irradiated submariners [4] but this was not replicated in the Netherlands [5,6]. Yeh et al found a decreased risk for sex-hormone sensitive cancers, postulating this could be due to irradiation of the pituitary [7]. But sparse record-keeping has meant any epidemiological studies rely on patient recollections and small populations.
Perhaps this foray into radium delayed development of the adenoidectomy; the 2011 UK tonsillectomy audit found that 70% of adenoidectomies were still being performed with curettes (although with modern anaesthesia and evidence-based patient selection criteria it is a much safer procedure). Suction diathermy and coblation are increasing in popularity, representing further evolution of the humble adenoidectomy.
References
1. Meyer W. On Adenoid Vegetations in the Naso-pharyngeal Cavity: their Pathology, Diagnosis, and Treatment. Med Chir Trans 1870;53(1):191-216.
2. Semon F. Speech made at the unveiling of the Wilhelm Meyer Monument, at Copenhagen. Laryngoscope 1997;107.
3. Adenoids and American School Hygiene in the Early 20th Century.
https://nyamcenterforhistory.org/2015/
03/10/adenoids-and-american
-school-hygiene-in-the-early-20th-century/
Last accessed 12 September 2019.
4. Kang HK, Bullman TA, Mahan CM. A mortality follow-up study of WW II submariners who received nasopharyngeal radium irradiation treatment. Am J Ind Med 2000;38(4):441-6.
5. Verduijn PG, Hayes RB, Looman C, et al. Mortality after nasopharyngeal radium irradiation for eustachian tube dysfunction. Ann Otol Rhinol Laryngol 1989;98(11):839-44.
6. Ronckers CM, Van Leeuwen FE, Hayes RB, et al. Cancer incidence after nasopharyngeal radium irradiation. Epidemiology 2002;13(5):552-60.
7. Yeh H, Matanoski GM, Wang Ny, et al. Cancer incidence after childhood nasopharyngeal radium irradiation: a follow-up study in Washington County, Maryland. Am J Epidemiol 2001;153(8):749‑56.