Cochlear implants have quickly become a widely used aid for hearing-impaired people. As these implants include metal elements, the choice of an appropriate imaging modality for patients carrying such devices should receive special attention. This is important due to image artefacts caused by metal parts and to potential complications after imaging.
When cone beam computed tomography (CBCT) was first introduced some 15 years ago, it was primarily used for dental imaging within a relatively small region of interest (ROI). As the research and development of this technology has advanced rapidly, CBCT is currently commonly used for imaging all of the dental anatomy. Besides dental applications, CBCT has started to gain popularity as the imaging modality of choice also for bony structures in the ear-nose-throat (ENT) area. In addition to greatly softening the artefacts caused by metal elements, CBCT is able to offer excellent bony delineation and high spatial resolution.
Indications
Assessment of postoperative imaging of patients carrying cochlear implantation should be done with great consideration, and CBCT is a viable alternative especially if postoperative complications are predicted. This judgment is demonstrated by two postoperative cases with cochlear implantation that showed complications in the processor part of the implant after undergoing magnetic resonance imaging (MRI) of other parts of the body.
Both of the patients were previously implanted with Nucleus Hybrid L24 cochlear implants. Patient 1 was imaged with one Tesla MRI due to a problem arising in the right knee (osteoarthritis) and patient 2 was imaged also with one Tesla MRI due to a prolapse suspected at level L4-L5. A recommended safety belt was wrapped around the implant area to keep the magnetic part of the implant in its position before imaging of the patient.
During MRI imaging the patients felt problems and pain in the temporal bone area, and the extra cochlear part of the implant was suspected to be deflected from its normal position.
“CBCT has started to gain popularity as the imaging modality of choice also for bony structures in the ear-nose-throat (ENT) area.”
Both patients were imaged immediately with CBCT using SCANORA® 3Dx (Soredex, Tuusula, Finland). The field of view (FOV) was 140 x 165 mm and voxel size 0.2 mm. Imaging parameters were 90 kV, 8 mA, 4.00s. Standard 1 mm axial, coronal and sagittal reformations were made, as well as MIP and 3D reconstructions using OnDemand3D™ software (Cybermed, Seoul, South Korea).
CBCT proved to be optimal for imaging of these implants because of the superior bony delineation and nearly artefact free images. All four parts, i.e. the receiver stimulation part, extracochlear electrode implanted on the surface of the temporal bone, the extracochlear electrode plate and the intracochlear electrode array could be well imaged with CBCT.
On CBCT all four of the important parts of the implant were very well seen both on the axial slices and three dimensional surface reconstruction images. The implant is placed on magnetic plates, and the extracochlear part was seen in an abnormal separated position. The intracochlear electrode array showed no signs of separation in either of the cases. The intracochlear electrodes were well seen in both of the cases.
The optimal images of these two patients are shown in the radiographic illustrations in Figures 1-7.

Figure 1: Patient 1 - Sagittal oblique reformatted CBCT image showing the intracochlear portion of the implant.
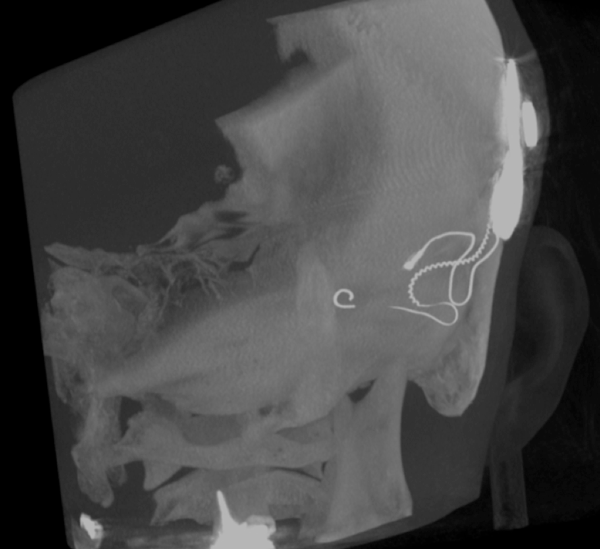
Figure 2: 3D MIP image of patient 1.
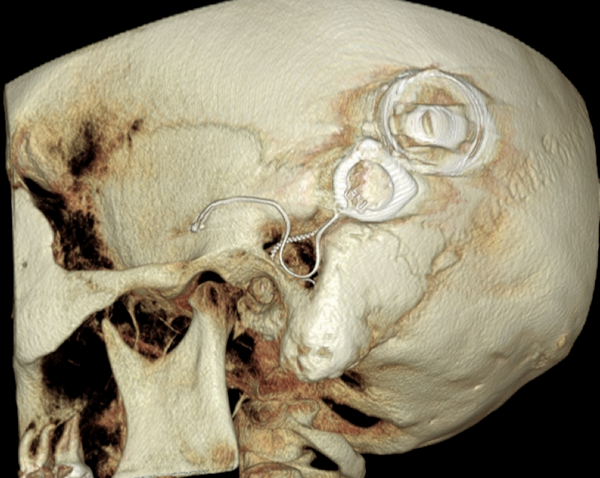
Figure 3: 3D reconstruction image of patient 1.

Figure 4: 3D MIP image of patient 2.

Figure 5: 3D reconstruction image of patient 2.

Figure 6: Sagittal thick MIP image of the implant of patient 2.
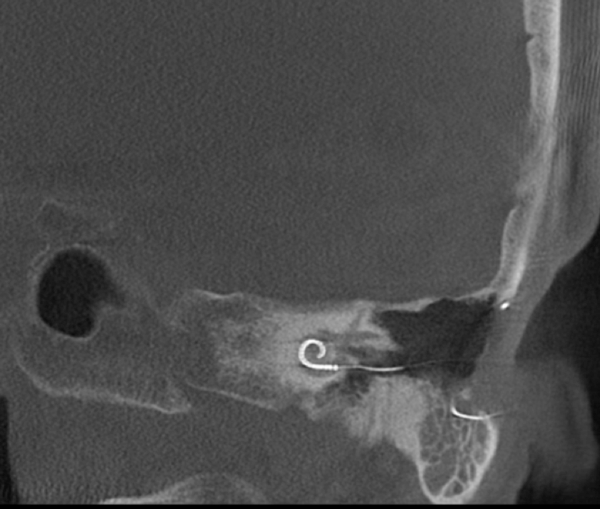
Figure 7: Patient 2 - Sagittal oblique image of the intracochlear portion of the implant.
Both patients underwent minor operations where the separated posterior portion was pushed back into its normal position.
Conclusion
As a conclusion, it may be recommended that after operation patients with cochlear implants should be imaged with CBCT and particularly, in case of suspected postoperative complications CBCT should be the imaging modality of choice. Because the radiation dose is so low compared to MDCT the use of CBCT is recommended instead of MDCT in these cases, and naturally a very careful fastening of a belt is preferred before MR imaging, if MRI is necessary at all.
HOW DOES IT WORK?
CBCT is an ideal imaging modality for postoperative imaging of patients with cochlear implants, because:
-
Radiation dose is considerably lower than with MDCT as the field-of-view (FOV) and location
can be optimised.
-
Spatial resolution in bony structures is excellent.
-
Images are nearly free of artefacts.
-
Examination is fast and convenient for the patient.


