Are we reaching a consensus on how hearing professionals should talk about hearing loss and dementia?
In 2024, the British Society of Audiology (BSA), in collaboration with the British Academy of Audiology (BAA) and the British Society of Hearing Aid Audiologists (BSHAA), published a position statement on adult-onset hearing loss (HL) and dementia.
Whilst much of the literature on this topic has been concerned with population risk, the focus of the position statement was on addressing individual risk in a clinical setting. The overarching aims of the guidance are to:
- Promote continuous professional development and ensure knowledge remains current.
- Support clinical and commercial practice that is grounded in evidence-based, critical thinking.
- Provide a framework to justify clinical decisions and actions, whilst supporting autonomous practice.
The main message in the guidance is that hearing interventions have proven benefits for improving hearing and communication. Hearing interventions help to keep the user cognitively and socially active, facilitating an active, engaged, independent and healthy older age. Essentially, hearing well allows us to grow, live and age well. However, the guidance cautions that there is no conclusive evidence that hearing loss causes dementia, nor that hearing interventions reduce the risk. The association between hearing loss and dementia should not be used as a justification for promoting use and sales of hearing aids.
"International publications reach similar conclusions: there is no conclusive evidence that hearing loss causes dementia or that hearing aids reduce the risk"
The BSA position statement has been widely disseminated and reported in a journal letter to raise awareness amongst the international hearing care community [1]. The position statement currently features prominently in internet search engines (e.g. Google search for ‘hearing loss and dementia recommendations’) suggesting it has high visibility and likelihood of being read and referenced.
The BSA et al statement [2] is consistent with the current views of the World Health Organisation [3], the umbrella review by Tang et al [4] and the Cochrane review on hearing aids for adults with mild and moderate hearing loss that is currently under review. There is insufficient evidence to recommend use of hearing aids to reduce the risk of cognitive decline in dementia. Whilst much of the earlier literature was concerned with population risk, highlighting an overall association between dementia and hearing (and, notably, many other factors), the focus of the BSA et al position was on individual risk and the fact that correlation does not mean causation. Whilst there is a statistical association between hearing loss and dementia, this should not be taken as evidence of causation [5]. There may be underlying factors that cause both dementia and multisensory loss, including hearing.
A recent article in The Hearing Review, a monthly resource for the hearing industry, outlined 10 recommendations for hearing professionals, encouraging the development of position statements and practice guidance addressing hearing and cognition [6]. Although this article did not cite the BSA et al statement or associated publications, it reached similar conclusions, provided similar guidance and used similar wording (see Table 1). We welcome the growing international consensus on a complex topic with ongoing uncertainties.
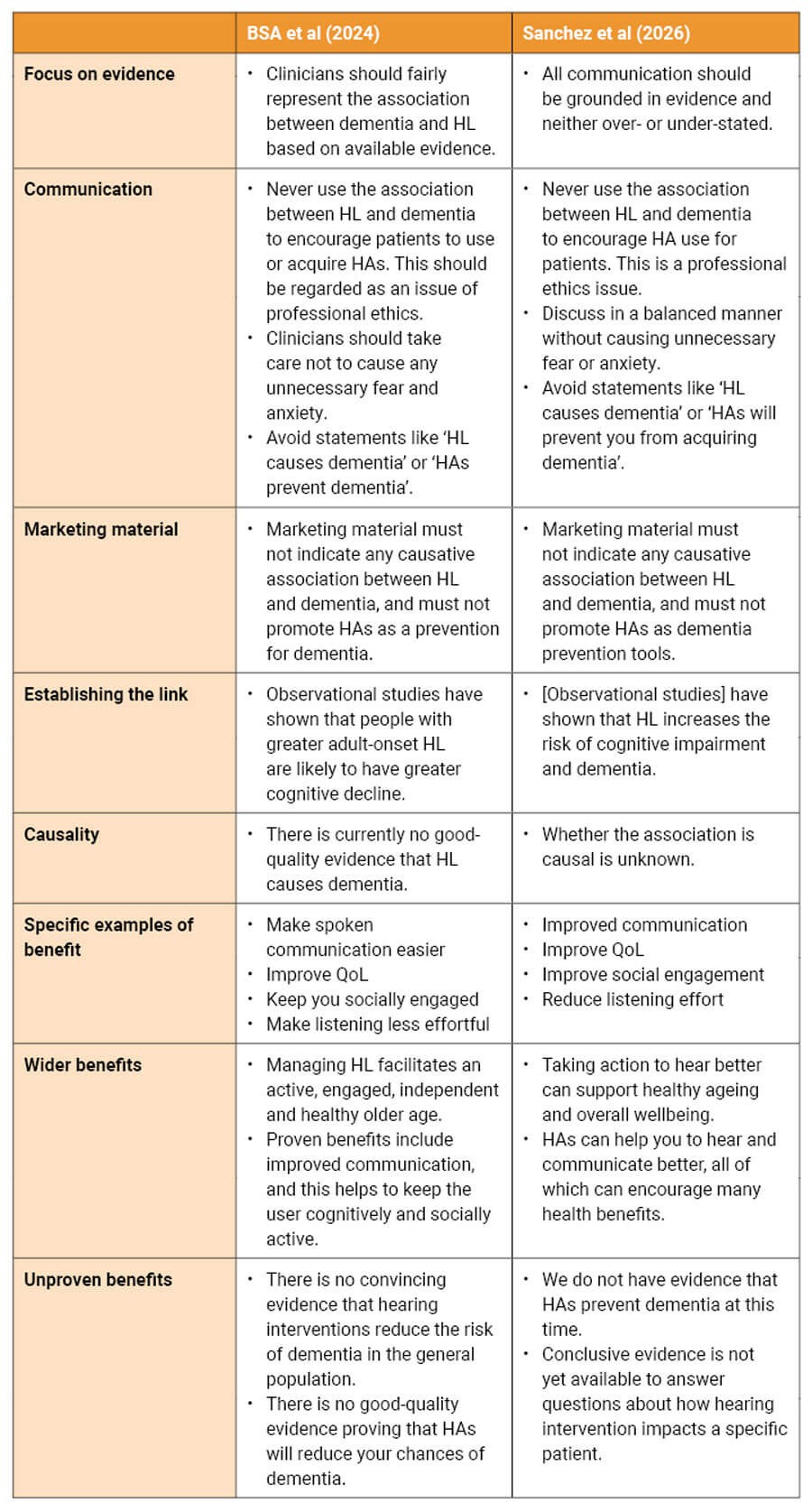
Table 1: Recommandations from BSA et al (2024) [2] and Sanchez et al (2026) [6]. Some statements have been paraphrased for brevity. (HL = hearing loss; HA = hearing aid).
Despite publication and dissemination of the BSA et al joint position statement, misunderstanding and misreporting persist regarding the nature of the relationship between hearing loss and dementia, and the individual risk. The BSA et al statement was based on an up-to-date summary of research evidence which has not changed substantially since 2024 and is reinforced by Sanchez et al [6]. Clear communication about the HL-dementia link can support realistic expectations and informed decisions. To support safe and effective practice within an appropriate scope, hearing care professionals are encouraged to familiarise themselves with this guidance (summarised in Table 1). Doing so will help ensure that their services, procedures, actions and clinical decisions remain professionally accountable.
No matter how well-intentioned, many publications stray away from the emerging international consensus and mistakenly equate correlation with causation, including some recent articles published in ENT & Audiology News. This error is sometimes compounded by the suggestion that audiologists should highlight a potential dementia risk to patients, which may cause significant harm, as a means of encouraging hearing-aid use. Both the UK and international guidance documents highlight that the association between hearing loss and dementia should never be used to persuade patients to acquire hearing aids and this should be regarded as an issue of professional ethics. In other words, it should be considered unethical to use dementia as a means to persuade a patient to use hearing aids because this has the potential to cause fear and significant emotional distress to a large number of people.
Clinicians should be aware that misleading comments may put them in professional jeopardy by failing to follow national guidance. Ultimately, the goal is to maintain high-quality, evidence-based patient care while ensuring that hearing care professionals practise within established professional and ethical boundaries.
References
1. Munro KJ, Dawes P, BSA, BAA and BSHAA. Explaining the link between adult-onset hearing loss and dementia to individuals with hearing loss. Int J Audiol 2025;64(8):861–2.
2. British Society of Audiology, British Academy of Audiology, the British Society of Hearing Aid Audiologists. The link between adult-onset hearing loss and dementia. 2024.
www.thebsa.org.uk/wp-content/uploads/
2024/11/Position-statement-HL-and-dementia
-a-guide-for-hearing-professionals-Nov-2024.pdf
[Link last accessed June 2026].
3. Chowdhary N, Barbui C, Anstey KJ, et al. Reducing the risk of cognitive decline and dementia: WHO recommendations. Front Neurol 2022;12:765584.
4. Tang D, Tran Y, Bennett RJ. The benefits of hearing aids for adults: a systematic umbrella review. Ear Hear 2025;46(3):563–70.
5. Dawes P, Munro KJ. Hearing loss and dementia: Where to from here? Ear Hear 2024;45(3): 529–36.
6. Sanchez V, Hickson L, Rich S, et al. Addressing cognition and hearing: 10 recommendations for HCP. 2026.The Hearing Review 2026.
Declaration of competing interests: KJM is director of the NIHR research for patient benefit programme. RW is employed by Diatec Diagnostics UK as Clinical Manager. This includes developing courses and training for a range of equipment provided by Diatec.






