The opportunities provided by mhealth technologies to personalise and encourage user involvement in hearing healthcare has many benefits for adults with hearing loss. Melanie Ferguson explains how mhealth can empower hearing aid users.
Connected health is likely to transform hearing healthcare – but what is it? Connected health is a sociotechnical model that uses remote technology to manage and deliver healthcare. Although there is no standardised definition for connected health, this is often considered as an overarching term that includes all aspects of telehealth, ehealth and mhealth, and can be viewed broadly as a combination of people, processes and technology.
Within the context of connected hearing healthcare, there has been a growing use of mhealth delivered by mobile devices (e.g. smartphones, tablets). mHealth technologies have the power to personalise hearing healthcare as well as increase user interaction, resulting in a more person-centred approach. These themes thread through a series of studies discussed here that examine hearing aid users’ experience of (i) smartphone-connected listening devices, and (ii) an mhealth programme to improve knowledge about hearing aids and communication. These technologies facilitate the user’s ability to control their listening device and personalise the information they need, which in turn leads to an increased sense of autonomy and empowerment.
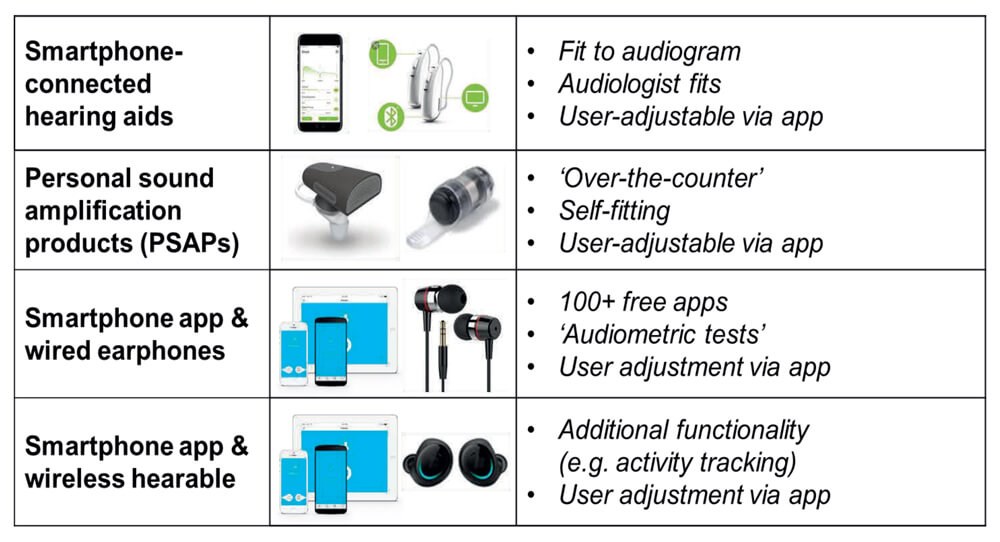
Table 1. Smartphone-connected device categories.
Smartphone-connected listening devices
The everyday experiences of adults with mild to moderate hearing loss were assessed after they trialled a range of smartphone-connected listening devices for several weeks in the real-world (see Table 1) [1,2]. First-time and existing hearing aid users from two studies (n=20, 44), average age of 65 years, were recruited from a publicly-funded UK NHS audiology service.
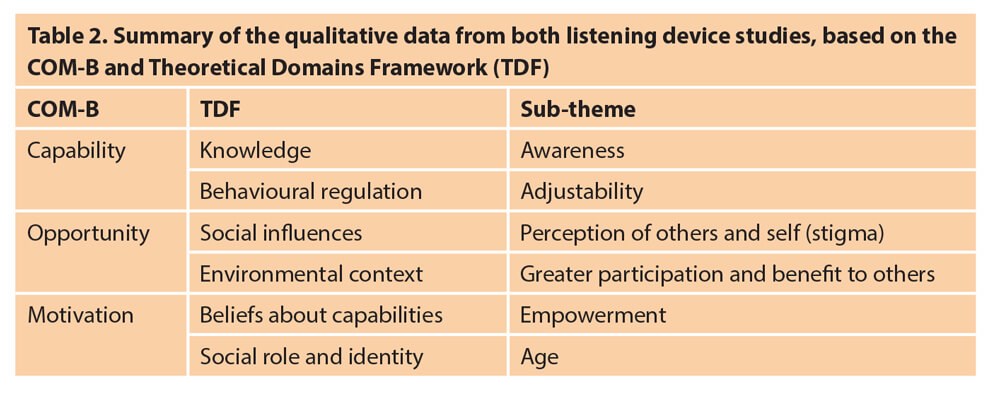
To identify health behaviours, semi-structured interviews and focus groups were analysed using a deductive thematic approach underpinned by the Theoretical Domains Framework (TDF). The TDF domains are linked to specific aspects of behaviour (B) from the COM-B model that comprises capability (C), opportunity (O) and motivation (M) to assess behaviour change (e.g. increase in hearing aid use) [3]. A summary of some of the key sub-themes or ‘active ingredients’ relating to the hearing devices is shown in Table 2.
User-controllability is key
A key advantage for smartphone-connected devices over conventional hearing aids was that the smartphone app gave the user control to fine-tune their device to meet their individual needs (capability). This was noted by all participants in one study, and 42% from the other study reported that user-control was the best feature of the app. One participant said, “The more you can adjust something and make it better for you, the better!”.
By being able to control the sound quality, participants were more likely to use their listening device and participate in conversations with others (opportunity). For example, one participant reported, “The app gave me a greater possibility of being able to hear what’s being said and join in.” Participants also reported that the smartphone helped reduce the stigma surrounding hearing aids as smartphones are a part of everyday life for most people.
For beliefs of capability (motivation), empowerment emerged as a key theme with participants reporting they felt more in control of their hearing as they could control and use their listening devices how and when they wanted. One participant noted, “It’s great. It gives you control…. it’s not other people running my life, it’s me.” Another participant said, “In a restaurant, it meant I didn’t have to sit with my back to the wall anymore – I could sit anywhere I wanted.”

mHealth education programme to improve hearing-related knowledge
High-quality education is one of five key components that promote successful self-management of long-term conditions. C2Hear is an online, freely available multimedia education programme co-designed with, and for, first-time hearing aid users (see C2hearonline.com). A large randomised controlled trial (RCT; n=203) showed multiple benefits. These included significantly better hearing-related knowledge, hearing aid handling skills, confidence in communicating, and higher hearing aid use [4].
A second RCT (n=43) showed significantly better self-efficacy for hearing aids when C2Hear was offered earlier at the hearing assessment [5]. Despite these positive outcomes, the non-personalised ‘one-size fits all’ approach had limitations including overly long videos and limited interactivity. To address this, C2Hear was repurposed for mobile technologies (m2Hear) to develop a personalised intervention to promote patient-directed self-management strategies [6]. This resulted in 42 short videos (approx. 1-2 min) that can be tailored to meet individual needs. Activities relating to hearing aids and communication were also embedded within the programme to increase user interaction. Each video was labelled with a specific question using wording that was co-developed with our study-specific patient and public involvement (PPI) panel, which acted as a guide as to which videos to watch (see Figure 1 for examples).
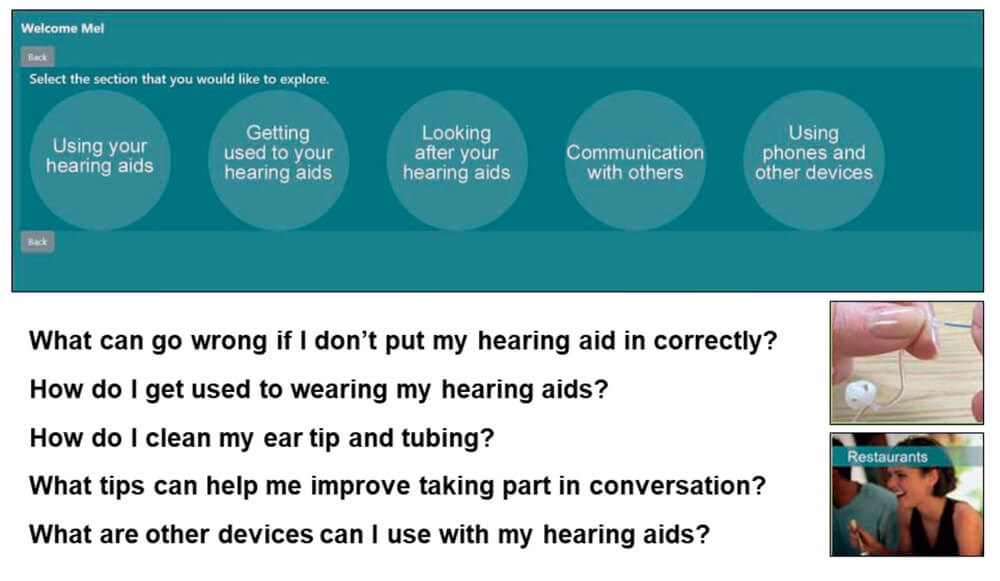
Figure 1. Screen shot from m2Hear and examples of questions linked to m2hear videos
from each of the five sections that represent progress along the patient journey.
m2Hear usability was high
m2Hear was most commonly used with tablets (40%), although nearly one third used more than one device (tablets 73%, smartphones 67%). Usability was measured using the System Usability Scale (SUS) and user-Mobile Application Rating Scale (uMARS; four subscales rated 1-5, where 5 is excellent). Usability for the SUS was high (M= 88.9%; >68 = above average), as was the overall uMARS score (M=4.2), and the Information (M=4.5) and Engagement (M=4.4) subscale scores. This indicated that m2Hear had very good, easy-to-use informational content, reflecting the PPI involvement during development.
Confidence and empowerment were enabled
Semi-structured interviews based on the COM-B indicated that m2Hear was a concise and comprehensive resource, and provided useful reminders and new information that facilitated knowledge of hearing aids and communication (capability). The use of mobile technologies made m2Hear simple and straight forward to use, and improved personalisation and accessibility (opportunity). Finally, m2Hear provided support and reassurance, improved confidence to self-manage hearing loss, and empowered participants (motivation). One participant said, “I haven’t got to rely on anyone else…I’d rather just be able to do it myself. If I’m constantly asking people, I just feel helpless, and I don’t like that.”
Empowerment within connected hearing healthcare
Mobile-delivered hearing interventions, which users can control themselves, have the power to improve participation, self-efficacy, autonomy and self-management. The theme of empowerment that emerged across all three studies has been shown in other healthcare areas, such as diabetes and mental health, to be associated with patient-centred care, self-management and self-efficacy. Enabling patients to assert control over factors that affect their health, such as health literacy, confidence and coping skills, leads to empowered patients. The use of the mhealth hearing technologies discussed here fits well with the concept of empowerment and resonates with the words ‘power’ and ‘freedom’, which are derived from the latin root for ‘empowerment’ (passe).
Self-efficacy is key to empowerment, as empowerment occurs when self-efficacy has been achieved. While self-efficacy is a concept that has been studied in the hearing literature, the concept of empowerment has received less attention. As the growth in connected hearing healthcare is likely to continue to grow at a rapid rate, further exploration of what empowerment means and how it can be measured is an enticing subject for future research.
References
1. Maidment D, Ali Y, Ferguson M. Applying the COM-B model to assess the usability of smartphone-connected listening devices in adults with hearing loss. Journal of the American Academy of Audiology 2019;30:417-30.
2. Habib A, Maidment D, Gomez R, et al. What are the benefits of smartphone-connected hearing aids in first-time and existing NHS hearing aid users? British Academy of Audiology Newsletter, Summer 2019;6-8.
3. Coulson N, Ferguson M, Henshaw H, Heffernan E. Applying theories of health behaviour and change to hearing health research: Time for a new approach. International Journal of Audiology 2016;55:S99-104.
4. Ferguson MA, Brandreth M, Brassington W, et al. A Randomized Controlled Trial to Evaluate the Benefits of a Multimedia Educational Programme for First-time Hearing Aid Users. Ear and Hearing 2016;27(2):123-36.
5. Gomez R, Ferguson M. (in press). Improving knowledge and self-efficacy for hearing aid self-management: the early delivery of a multimedia-based education program in first-time adult hearing aid users. International Journal of Audiology.
6. Ferguson MA, Maidment DW, Henshaw H. Gomez R. Knowledge is power: improving outcomes for patients, partners and professionals in the digital age. ASHA Perspectives SIG7 2019;58(4):1-9.
Declaration of Competing Interests: Some of the research reported in this article was funded by Phonak and the NIHR.
Acknowledgements
Many thanks to my colleagues David Maidment, Rachel Gomez and Alia Habib who made significant contributions to this research when we worked together at the NIHR Nottingham Biomedical Research Centre. Thanks also to Claire Benton, Will Brassington and staff at the Nottingham Audiology Services. This article presents independent research funded by Sonova A/G and National Institute of Health Research (NIHR). The views are those of the author and not necessarily those of the NHS, the NIHR or the Department of Health.



