One important aspect of the new paradigm in tinnitus research is to question basic assumptions. What associations does the sex of a person have with their experience of and reaction to tinnitus? Chris Cederroth raises the question and tells us how we can move towards the answers.
A number of medical research agencies have started to incorporate policies in their funding calls to encourage the inclusion of sex and gender aspects in the projects they support - e.g. National Institutes of Health (NIH), Canadian Institutes of Health Research (CIHR), the Swedish Research Council. As medical care progressively gears towards personalised medicine, it is increasingly recognised that sex will become a key feature for optimising treatments.
Sex differs from gender in that it refers to the biological classification (what is encoded in our genes), while gender refers to the social roles. Historically, a large number of pre-clinical studies were focused on one sex, potentially based on beliefs that fundamental mechanisms do not differ between sexes, that female hormones largely influence the outcomes, and that considering sex as a variable substantially increases the number of resources. One consequence of having neglected the consideration of sex as a biological variable in pre-clinical studies, was the withdrawal of 80% of drugs (between 1997 and 2000, in the US market) due to greater risk of adverse reactions in women than in men. However, sex-specific mechanisms have great potential for innovation as evidenced in research on genetics, neuroscience, and immunology, among others.
“Historically, a large number of pre-clinical studies were focused on one sex, potentially based on beliefs that fundamental mechanisms do not differ between sexes”
Tinnitus does not escape the rule: pre-clinical research is mostly unisex, whereas clinical research – while it incorporates both males and females – sex differences are seldom investigated. Among the first large epidemiological studies that have investigated sex effects, is the cross-sectional study from Nondahl et al 2010 [1] who reported a lower risk for tinnitus in women with past alcohol consumption (odds ratio (OR) = 0.56; 95% confidence intervals (CI): 0.35-0.90) in contrast to men (OR = 1.33; 95% CI: 0.70-2.51), and reversely a greater risk for tinnitus in men with a history of ear infections (OR = 1.75; 95% CI: 1.20-2.57) in contrast to women (OR = 0.90; 95% CI: 0.62-1.31). However, the sex-stratified analyses were not consistently applied through all variables and thus it remains unclear how sex would have impacted all other variables investigated in the study.
TIGER – tinnitus genetic and environmental risks
Funded by the EU GENDER-NET ERA-NET (www.gender-net.eu/?lang=en; http://gender-net-plus.eu), TIGER (https://tiger.tinnitusresearch.net) aims at better understanding the impact of sex on tinnitus in humans. Four participating countries form the consortium, with Sweden (Karolinska Institutet) as a coordinator, and Italy (Mario Negri Institute), Spain (GENYO, Granada), and Norway (Bergen University) as main recipients. The project was based on an increasing amount of evidence pointing towards differences between men and women with tinnitus, the latter showing higher anxiety, stress and hyperacusis, making it a greater emotional burden (Figure 1) overall, affecting life quality [3] and potentially contributing to greater risk in suicide attempts [4].
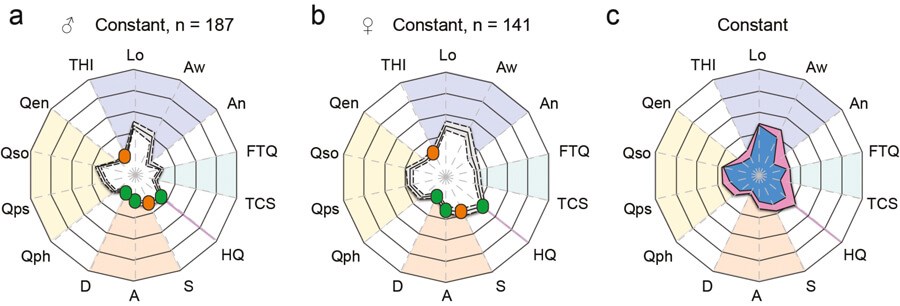
Figure 1. Radar chart profiling for characterising global health burden in individuals with constant tinnitus. Radar charts illustrating the evaluation of global changes in tinnitus burden according to constant tinnitus for men (a) and women (b). In these charts, a solid line shows the average, with the 95% confidence intervals represented by the dashed lines. Average tinnitus-associated burden, for men (blue) and women (pink) is shown for constant (c) tinnitus. Instruments are labelled as follows: THI: tinnitus-related psychological distress; Lo: Tinnitus loudness; Aw: Tinnitus awareness; An: Tinnitus annoyance; TCS: Tinnitus catastrophising; FTQ: Tinnitus fears; HQ: hyperacusis questionnaire; S: Stress; A: Anxiety; D: Depression scores; Quality of Life for physical (Qph), psychological (Qps), social (Qso), and environment (Qen). Colour dots illustrate the severity score of those instruments with published severity category boundaries: negligible (green), moderate (orange), severe (red). Image adapted from Schlee et al [2].
Reversely, while women’s psychological health appears more impacted by tinnitus than in men, it remains unclear if this is also accompanied with greater risk in accompanying comorbidities. For instance, it has been previously reported that headaches and hyperacusis are more frequent in women with tinnitus, but this appears to be due to the fact that headaches and hyperacusis are simply more frequent in women than in men in the general population. As a consequence, the risk for tinnitus when accompanied by either headaches or hyperacusis, does not differ between men and women [5,6].
“The project was based on an increasing amount of evidence pointing towards differences between men and women with tinnitus, the latter showing greater anxiety, stress and hyperacusis”
Objectives
With accumulating evidence that tinnitus is influenced by genetic factors, a search for genetic variants associated with tinnitus was required. TIGER aims at analysing and computing the interrelationship between non-genetic as well as genetic risk factors for tinnitus. Specific emphasis is put on the question, how a combination of risks jointly shifts the regulation of cellular pathways towards a diseased state. TIGER hopes to establish a basis for creating a risk score that will eventually allow the community to assess the tinnitus risk more accurately, to determine future diagnostic and therapeutic opportunities, and to generate clinical guidelines for the medical management of high-risk severe tinnitus patients.
Task 1 - To identify novel environmental risk factors for developing tinnitus in each gender.
Task 2 - To identify potential genetic determinants for tinnitus in each sex.
Task 3 - To identify genetic and environmental interactions that synergistically increase risk for tinnitus for each sex and gender.
Task 4 - To identify potential blood biomarkers for tinnitus for each gender.
Task 5 - To generate predictive algorithms based on the collected data.
Progress
Thanks to the development of the Swedish Tinnitus Outreach Project (STOP) (https://stop.ki.se), which now consists of 7943 registered participants, with 5500 sets of individual questionnaire data, and near 1000 individual audiological measures performed (half from tinnitus sufferers, the other half from subjects without tinnitus), epidemiological studies are underway. With plasma and DNA available for nearly 80% of participants, genetic and blood biomarkers can now be associated with highly phenotyped tinnitus traits. A proteomic screen on 1000 constant tinnitus cases and non-tinnitus controls was performed using Proximity Extension Assay (PEA) from O’LINK, which is an extremely sensitive multiplex assay covering 96 proteins. In parallel, 97 cases with tinnitus as a big problem (based on the tinnitus functional index cut-offs) were submitted to whole genome sequencing and compared against 1000 samples from SWEGEN. Analysis of both biomarker datasets is ongoing.
Conclusions
TIGER leverages on a large deep-phenotyping study such as STOP, which will give rise to unprecedented data in the tinnitus field, and that may guide into means of determining tinnitus subtypes using blood and DNA biomarkers. Given the increasing relevance of sex as a biological variable for research and innovation [7], we hope that TIGER will bring new knowledge that will guide towards personalised medicine. However, stratification by sex and by tinnitus subtypes dramatically reduces statistical power, which emphasises the need of global hearing and tinnitus registries. International collaboration is a necessity. Once established, it may help in addressing emerging needs such as the current COVID-19 pandemic, the impact of which on hearing loss and tinnitus remains to be determined.
References
1. Nondahl DM, et al. The ten-year incidence of tinnitus among older adults. Int J Audiol 2010;49:580-5.
2. Schlee W, Hall DA, Edvall NK, et al. Visualization of Global disease Burden for the optimization of patient Management and treatment. Front Medicine 2017;4(86):6.
3. Schlee W, Hall DA, Edvall NK, et al. Visualization of Global Disease Burden for the Optimization of Patient Management and Treatment. Front Med (Lausanne) 2017;4:86.
4. Lugo A, Trpchevska N, Liu X, et al. Sex-Specific Association of Tinnitus With Suicide Attempts. JAMA Otolaryngol Head Neck Surg 2019;145(7):685-7.
5. Lugo A, Edvall NK, Lazar A, et al. Relationship between headaches and tinnitus in a Swedish study. Scientific reports 2020;10(1):8494.
6. Cederroth CR, Lugo A, Edvall NK, et al. Association between hyperacusis and tinnitus. Journal of Clinical Medicine 2020;in press.
7. Danska JS. Sex matters for mechanism. Sci Transl Med 2014;6(258):258fs40.
Declaration of Competing Interest: The author is supported by the UK National Institute for Health Research (NIHR) but his views herein are his own and do not represent those of NIHR nor the UK Department of Health and Social Care.



