Hearing impairment is one physical disability that is increasing in prevalence in society in general, and in older adults in particular. Approximately 34 to 36 million Americans report suffering from some degree of hearing impairment with the number rising to 52.9 million by the year 2050. Extrapolating from a number of population based studies, hearing loss prevalence ranges from 30-47% among persons 65+ years and 70-80% for those 80 years of age and older [1].
Often assumed to be benign, hearing loss is an insidious condition which has profound effects on quality of life; age-related hearing loss (ARHL) takes about 7-10 years before people first realise that the condition exists. The inability to communicate effectively, often robs individuals of being productive members of society. ARHL is indirectly associated with mortality and directly associated with functional disability, social isolation, poor self-reported health and depression. Hearing impairment is a risk factor for cognitive decline, falls and mobility decline, and individuals with hearing loss have the increased burden of medical comorbidities.
Hearing loss is independently associated with increased burden of disease, poorer self-reported health, increased odds of hospitalisation, and healthcare use [2]. It has recently been acknowledged that on hospital discharge, errors often result from a breakdown in communication between the hospital team and the patient or primary care physician. As hearing loss is often invisible to primary care physicians, errors and adverse events in discharge planning which have been attributed to breakdowns in communication could be due, in part, to unrecognised hearing loss [3]. For example, upon discharge, physicians tend to rely on verbal instructions and the entire interaction is typically rushed [3]. Identification of persons with hearing loss may contribute to more effective transitions of care, notably, greater clarity in physician–patient communication, and adoption of strategies to promote communication, potentially contributing to reductions in medical errors in discharge planning.
“Age-related hearing loss remains virtually untreated in the majority of older adults.”
A highly stigmatised condition for which people are reluctant to pursue treatments, hearing loss remains virtually untreated in the majority of older adults [4, 5]. Hearing aids are increasingly more sophisticated with features designed to improve speech understanding in noise, the most common complaint of individuals pursuing hearing aids. With the advent of hearing assistive technologies, including personal sound amplifiers, inexpensive alternatives open the door to numerous options from which to choose, especially for individuals who may not be ready or are unable to afford digital hearing aids.
Since hearing loss is prevalent and a range of effective interventions are available, screening at-risk older adults for hearing loss should become a priority in primary care. Identifying persons with hearing loss can potentially reduce illness burden, promote provision of high quality care and more effective care transitions. Acknowledging the importance of hearing status, the Medicare-covered Annual Wellness Visit (AWV) includes provision of Personalised Prevention Plan Services (PPPS) at no cost to the beneficiary.
Key elements of the first AWV providing PPPS include, among other things, detection of any cognitive impairment, review of potential risk factors for depression, review of functional ability based on direct observation or any appropriate screening questions or a screening questionnaire including at a minimum assessment of ‘hearing impairment, ability to successfully perform activities of daily living ( ADLs), fall risk and home safety’ [6]. The existence of a potential hearing loss can be detected with a high degree of accuracy via direct questioning, handheld audiometry, and / or through observation of subtle behavioural indicators (Table 1) [7, 8]. Figure 1 shows a sample form which could be adapted for use when conducting hearing screenings. As a supplement to a hearing screen, when hearing loss is suspected, it is important to provide written and oral instructions and to adopt communication strategies such as facing the patient when speaking, in an effort to promote compliance and effective care transitions.
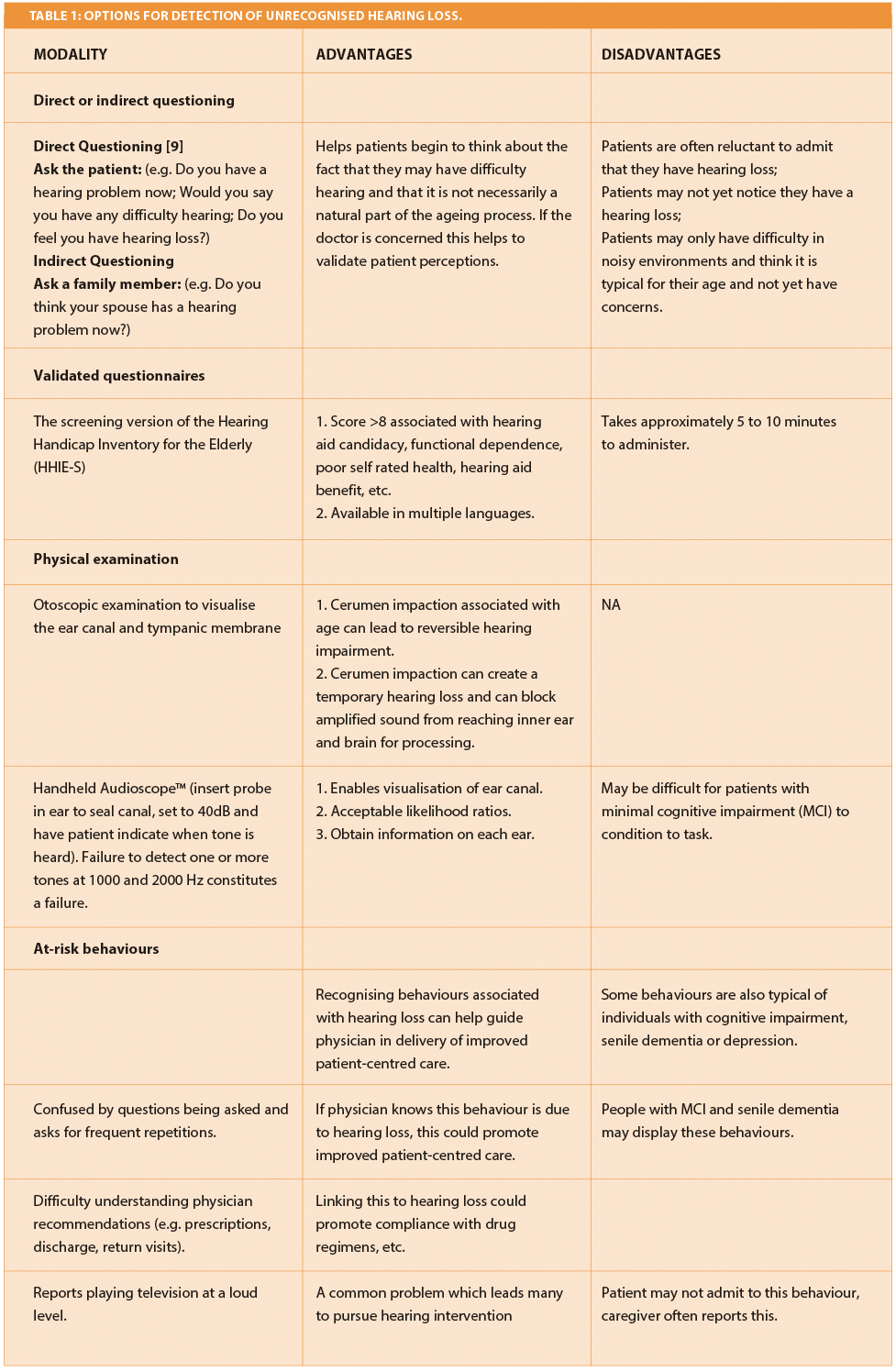
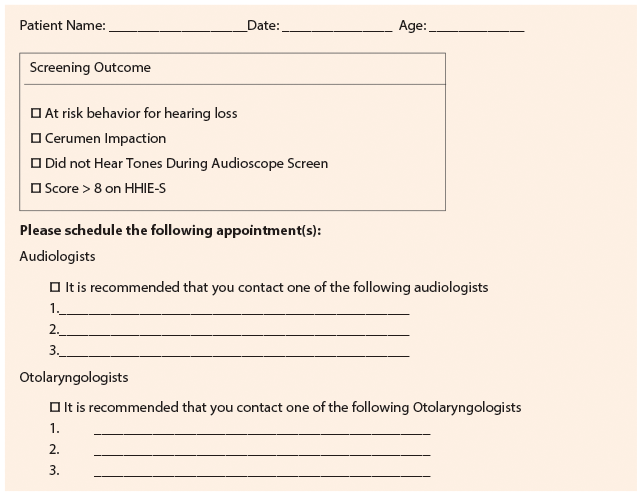
Figure 1: Sample Referral Form.
In summary, an underestimated public health problem, hearing loss is a serious threat to functional independence, quality of life and health of older adults. Mounting evidence suggests that a range of effective interventions is available to remedy hearing loss and its negative effects, yet 23 million Americans with hearing loss do not utilise hearing aids [4]. Routine screening of individuals at risk for hearing loss, including individuals at risk for falls, persons with depression, or memory problems, has the potential to reduce the burden of illness posed by hearing loss and improve health care outcomes [10].
References
1. Weinstein B. Geriatric Audiology – 2nd Edition. New York, USA; Thieme Medical Publishers Inc; 2012.
2. Genther D, Frick K, Chen D, Lin FR. Association of hearing loss with hospitalization and burden of disease in older adults. JAMA 2013;309:2322-4.
3. Kripalani S, Jackson A, Schnipper J, Coleman E. Promoting effective transitions of care at hospital discharge: a review of key issues for hospitalists. J Hosp Med 2007;2:314-23.
4. Chien W, Lin FR. Prevalence of hearing aid use among older adults in the United States. Arch Intern Med 2012;172:292-3.
5. Hogan A, Byrne D, Reynolds K. (2010). Beyond the gap: Towards a more comprehensive structuring of hearing services. ENT & Audiology News 2012;19:79-83.
6. Medicare Learning Network (MLN) Providing the Annual Wellness Visit (AWV). 2012:
http://www.cms.gov/Outreach-and-
Education/Medicare-Learning-Network-MLN/
MLNProducts/Downloads/Annual
WellnessVisit-ICN907786.pdf
Last accessed March 2014.
7. Pacala J, Yueh B. Hearing deficits in the older patient; “I didn’t notice anything”. JAMA 2012;307:1185-94.
8. Chou R, Dana T, Bougatsos C, et al. Screening for Hearing Loss in Adults Ages 50 Years and Older: A Review of the Evidence for the U.S. Preventive Services Task Force [Internet]. Rockville, USA; Agency for Health Care Research and Quality (US); 2011: Report No 11-05153-EF-1.
9. Gates G, Murphy M, Rees T, Fraher A. Screening for handicapping hearing loss in the elderly. J Fam Pract 2003;52:56-62.
10. Bagai A, Thavendiranathan P, Detsky AS. Does this patient have hearing impairment? JAMA 2006;295:416-28.
Declaration of Competing Interests: None declared.


