There are international drivers focusing our attention on measuring outcomes; Anthony Hogan looks at the data to see how we are currently measuring up.
Introduction
A global paradigm change is impacting on the provision of disability services. At its heart, the change stems from the proclamation of the United Nations Convention on the Rights of Persons with Disabilities (2008), to which some 160 countries are signatories [1]. This Convention, coupled with the administrative tools that are being developed and implemented in jurisdictions across the world [2], focus on three key principles:
- People with disability have choice and control over the services provided to address individual need
- A focus on measurable outcomes
- Enhancing the social equality of people with disabilities.
Brought to bear on the practice of audiology today, the United Nations Convention on the Rights of Persons with Disabilities signals a paradigm change in the provision of hearing services [3]. This change will have impacts in hearing services far beyond notions of client centred therapy. It will involve the necessity ensuring that our clients are educated about the services being offered so that they can demonstrably make an informed choice about the nature and range of hearing services or devices provided to them.
It will require the industry collectively, and practitioners individually, to be able to empirically demonstrate that the services offered really do make a difference in a person’s life specifically, and for hearing impaired people generally. In this context, making a difference does not really refer to audiological concepts such as insertion gain, but to indicators about personal wellbeing and social participation. This is because the indicators associated with evaluating services within the context of the new paradigm are social and economic in nature. They are concerned about service:
- Impacts, e.g. do people use their hearing aids; can they communicate?
- Outcomes, e.g. social inclusion, social participation and individual wellbeing
- Efficacy and efficiency, e.g. the comparable benefit to the sector given the range of expenditures incurred.
In this article I present some data that may serve as an indicator of where we are at presently in terms of measurable client outcomes and social equality. And in so doing, this article in turn provides an opportunity to consider the size of the challenge the shift in paradigm may have for the audiological industry.
Results
Most people in this sample (70%) reported being satisfied with their life overall. A majority (73%) also rated their health as good or better (Figure 1). Similarly, 73% rated their hearing as good or better (Figure 2). Of those who rated their hearing as fair or poor (27%), 46% of those aged less than 65 years were in the workforce. Hearing aid owners, whose hearing was fair to poor, reported fair to poor health (X2 (4)=1018.7; p<.001).

Figure 1. Self-rated health.
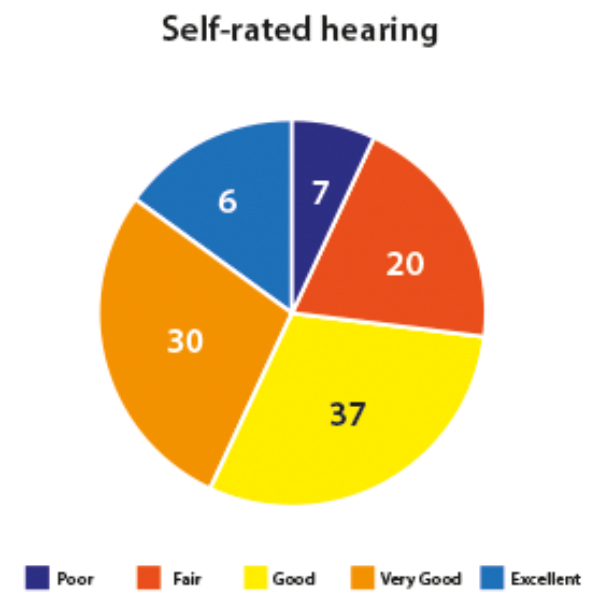
Figure 2. Self-rated hearing.
Data was provided on the extent to which people who answered questions on their hearing experienced hearing communication difficulties in everyday life. Across the responses it can be seen that a quarter to a third of people report distinct difficulties. For example, 7% of all people report regular difficulties in hearing the radio or television; 8% of people report regular difficulties in hearing while in the car; and 5% of people report regular difficulties in hearing while at the movies. Lastly, 10% of people report regular difficulties hearing in social settings.
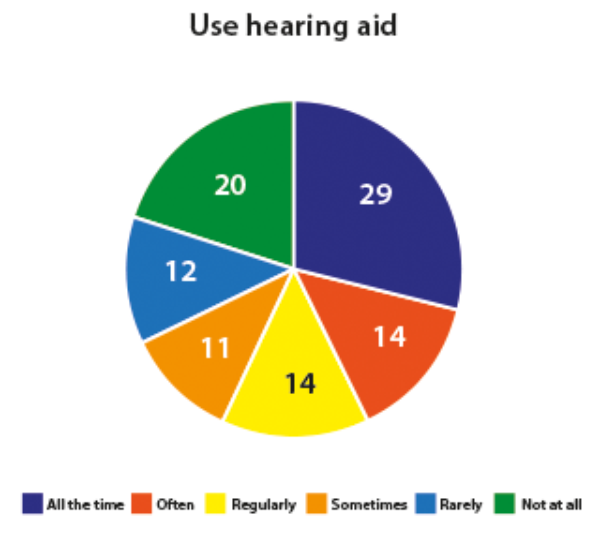
Figure 3. Hearing aid usage.
Within this sample, 15% of people aged 50 years and over reported owning a hearing aid. People who used hearing aids frequently, reported average daily use of approximately eight hours per day. It is noted however, that 32% of people owning a device rarely if ever used it (Figure 3). Hearing aid usage, as shown in Table 1, increases with age.

Hearing aid use was associated with self-rated hearing difficulties with 73% of those who rated their hearing as poor and 35% of those who rated their hearing as fair, owning a device (X2 (4)=1,018.7; p<.001). The level of hearing aid use was also associated with self-rated hearing difficulties with 43% of those who rated their hearing as poor and 23% of those who rated their hearing as fair using their device daily (X2 (15)=39.6; p<.001).
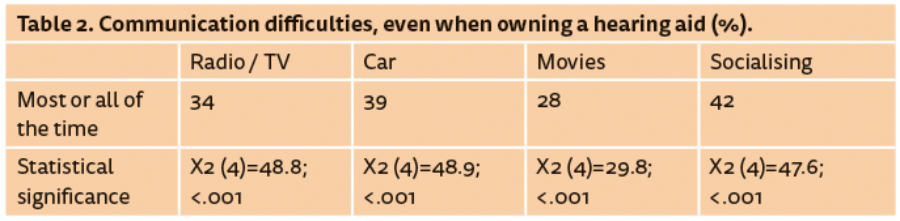
Of the people who rated their hearing as fair or poor, and owned a hearing aid, a significant proportion still experienced day-to-day communication difficulties. Most notably, as shown in Table 2, some 42% experience difficulties hearing in social settings most, if not all of the time.
Discussion
This study found that 15% of people aged over 50 years, owned hearing aids. Of these, some 2:3 people routinely used their devices. However, even with the benefit of hearing aids, a large proportion of people whose hearing is fair or poor, still experienced significant difficulty hearing in everyday communication settings, i.e. they faced barriers to social inclusion and participation. Indeed, the level of residual disability amongst device users is very concerning as it raises the question of the extent to which existing service models, particularly those which are device-centric, adequately address the needs of today’s clients.
The reported rates on non-device usage also raise significant economic concerns from both an individual and from a third-party payer perspective. Of course, data on non-device usage is highly contentious because figures on non-usage vary with the nature of questions being asked and the research methods being used. It will become increasingly important, however, that independent studies such as these continue so that the community can have confidence when industry performance data is reported. Economic and social concerns are also evident with regards the rates of workforce participation amongst deaf and hearing impaired people. The workforce participation rate of those aged less than 65 years reported in this study (46%) was considerably lower than that of its comparable population (65%) [4]. It is hardly surprising then that significant economic studies identify the economic costs of lost productivity, as a significant issue impacting on the sector [5].
At a population level, this study suggests that people with impaired hearing do not enjoy social equality and that they face specific and significant barriers to social inclusion, even when using hearing devices. This study also demonstrates that social factors associated with hearing impairment are measureable. What is also evident is that in an era of outcomes-focused service provision, the broader efficacy of hearing services will come increasingly into question. It may well be that a change in service paradigm involves not only a change to service evaluation, but also a change in the way services are delivered generally.
About this study
The data reported in this paper were collected by an independent Australian market research company, Instinct and Reason. The data were collected over a series of 13 consecutive surveys between 2013 and 2016, with each sample consisting of approximately 1000 people. In three waves of this study, respondents were asked about their experiences of hearing and device usage. The author expresses his thanks to Instinct and Reason for enabling him to access these data without charge. The total sample for this study was n=13,591. The sample of males and females was approximate to the population (males 51%, females 49%). Within the sample respondents were aged:
- 50-54 years = 15%
- 55-64 years = 37%
- 65+ years = 48%
The sample of people completing questions in relation to hearing was n=3085. Respondents were asked to report on their health, hearing, hearing aid usage and experiences of difficulties in everyday communication settings.
References
1. United Nations Division for Social Policy and Development Disability. Convention on the Rights of Persons with Disabilities (CRPD). United Nations; 2016;
https://www.un.org/development/desa/
disabilities/convention-on-the
-rights-of-persons-with-disabilities.html
Last accessed 10 November 2017.
2. Australian Department of Human Services. National Disability Insurance Scheme.
https://www.ndis.gov.au
Last accessed 10 November 2017.
3. Hogan A, Phillips R. Hearing impairment and Hearing disability – towards paradigm change in hearing services. London, UK; Ashgate; 2015.
4. Australian Bureau of Statistics. Labour Force, Australia, monthly figures.
http://www.abs.gov.au/
ausstats/abs@.nsf/mf/6202.0
Last accessed 10 November 2017.
5. The National Foundation for the Deaf. Social and economic costs of hearing loss in New Zealand. Deloitte Access Economics; 2016;
https://www2.deloitte.com/content/dam/
Deloitte/au/Documents/
Economics/deloitte-au-economics-social-economic
-cost-hearing-loss-new-zealand-021216.pdf
Last accessed 10 November 2017.
Declaration of competing interests
Anthony Hogan has worked as a research and training consultant for Instinct and Reason.



