Since the start of the COVID-19 pandemic we have seen an exponential increase in the use of face masks. Guidance around the globe varies on the use of face masks as an effective barrier to the coronavirus. Whereas in pre-covid times, masks were limited to use in specific occupational settings, mask-wearing is now common-place in all public settings.
Public Health England’s guidance advises the use of face masks in particular scenarios in clinical practise, with guidance from ENT UK and joint guidance from the UK audiology bodies (BAA/BSA/BSHAA/AIHPP) giving specific approaches for our clinical settings.
Patient groups and hearing care professionals have long challenged and advocated for better deaf awareness in medical settings, with some of this concern due to the use of face masks and the inability to lip-read. The advent of this pandemic has set a new normal which further challenges the hearing impaired.
Professor Kevin Munro and Dr Michael Stone from Manchester University are leading the way in highlighting the challenges of face mask use for the hearing impaired. Professor Munro’s article, first published in The Conversation, has gained international attention, and Dr Stone’s recordings give voice to the scale of the speech-communication difficulties. In addition to these, below you will also find a link to a podcast from the Manchester Centre for Audiology and Deafness, in which Kevin Munro discusses the effects of facemasks on speech understanding.
It is incumbent on hearing healthcare professionals to practise and advocate for good communication tactics. A number of solutions are being developed and tested such as facemasks with a clear window to aid lip-reading and real timing speech to text apps. With such as dynamic environment I’m sure many more solutions are yet to come!
Gareth Smith, Audiology Editor, ENT & Audiology News.
![]()
Face masks are a challenge for people with hearing difficulties
This article is republished from The Conversation (https://theconversation.com)
under a Creative Commons license. You can find the original article at:
https://theconversation.com/face-masks-are-a-challenge-for-people-with-hearing-difficulties
The use of face masks by the public is a controversial topic and not supported by the World Health Organization [1]. Evidence suggests that while face coverings and surgical masks can prevent large particles spreading from an infected person wearing a mask to someone else, they don’t trap tiny particles such as coronavirus [2]. A mask may also increase a person’s risk of contracting COVID-19 by encouraging them to touch their face as they fit and adjust it. Exhaled air can irritate the eyes, which might also tempt the wearer to wipe them.
On the other hand, wearing a mask may stop people with coronavirus spreading it to others (although the evidence for this is currently weak). As governments search for a surefooted transition to whatever the new norm will be, there is a danger that a policy of encouraging the public to wear face masks may precede the evidence.
Unintended consequences
It’s important to consider some of the unintended consequences. Wearing a face mask may impair the ability for some people to communicate with ease because it prevents lip reading and it can reduce the level of speech transmitted from the mouth. At the very least, removing visual cues can make communication more taxing because of the mental exertion required to listen, especially when there is background noise. As a result, even if a person can follow what is said, they have fewer mental resources left to think about and recall what they heard.
Research has shown there are beneficial effects of wearing surgical masks made from a transparent material that allows the mouth to be seen [3], but these aren’t widely available. And there have been calls for the public to use transparent face shields [4], rather than masks, which may offer a solution. But the public has yet to adopt this solution.
The increased effort needed to listen and communicate is exacerbated in people who have a hearing loss [5]. According to the WHO, there are 1.33 billion people globally with hearing loss. Hearing loss leads to communication difficulties between family members, colleagues and friends. It is associated with negative factors [6] such as poor social interactions, isolation, depression and anxiety, increased risk of dementia and reduced quality of life. In fact, there are probably many people with hearing loss who were able to manage but would struggle with the widespread use of masks.

Mask misery
An unintended consequence of wearing a face mask might be that social distancing is replaced with social isolation and poor mental wellbeing in older adults with hearing loss. A huge section of society could be subjected to mask misery. It is also not clear whether wearing a face mask provides a false reassurance about risk reduction (encouraging people to relax behaviours that are known to interrupt transmission, such as keeping at least two metres apart), or if it acts as a reminder to steer clear of people.
Coronavirus tends to take a more severe form in older people [7] many of whom are likely to suffer from hearing loss. This means that those admitted to a hospital are especially vulnerable.
The N95 and FFP3 respirator masks for frontline health and care workers can filter 95% of tiny particles [8], but they are much more likely to distort and reduce the level of speech. This makes communication particularly difficult at a time of heightened anxiety and when the content of conversations is novel and unpredictable. Imagine the apprehension of being greeted by someone in full PPE wearing a fitted mask and muffled speech competing with the hiss of oxygen from a breathing mask or nasal cannula.
Practical advice for the hard of hearing
So what can you do to improve communication if you have a hearing loss and are confronted by someone wearing a face mask?
- Ask them to reduce the background noise as much as possible or move to a quieter location.
- Ask them to talk slowly and not shout.
- If you have a hearing aid, make sure to wear it.
- Some hospitals provide portable hearing amplifiers to help with communication if you have lost your hearing aid or it has stopped working.
- If you don’t have a hearing aid but need one, you can always download a hearing aid app to your mobile phone that can provide amplification to improve speech understanding. Or you can find an app that translates speech into text in real-time.
References
1. https://www.theguardian.com/world/2020/apr/07/face-masks-cannot-stop-healthy-people-getting-covid-19-says-who
2. https://annals.org/aim/fullarticle/2764367/effectiveness-surgical-cotton-masks-blocking
-sars-cov-2-controlled-comparison
3. https://www.ncbi.nlm.nih.gov/pubmed/28054912
4. https://jamanetwork.com/journals/jama/fullarticle/2765525?guestAccessKey=6af59d69-940c-49d68fc3d790577a6a48&utm_source=For_ The_Media&utm_medium=referral&utm_campaign=ftm_links&utm_content=tfl&utm_term=042920
5. https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(16)31678-6/fulltext
6. https://bmjopen.bmj.com/content/8/7/e021502
7. https://theconversation.com/why-are-older-people-more-at-risk-of-coronavirus-133770
8. https://www.cleanairresources.com/resources/respirator-vs-face-mask-what-s-the-difference
This article is republished from The Conversation (https://theconversation.com) under a Creative Commons license.
![]()

Quantifying the scale of speech-communication difficulties
while wearing face protection
A recent article in the BMJ raised the issue of the wearing of face masks by the wider public, and the possible effects on reduced transmission of COVID-19 [1]. A response by Lazzarino raised several possible issues, one being that of impeded speech communication due to a face covering [2].
Success in speech communication relies on many factors, mostly acoustic, but some visual. These factors depend on both talker and listener. For the talker, the acoustic-related factors include the clarity of enunciation, the vocal effort used, and the relative orientation between talker and listener. For the listener, the acoustic factors affecting success include degree of hearing impairment, distance from talker, level of background noise, familiarity with, and context of, the vocabulary being used, and possibly listening to a non-native language.
One visual cue for the listener, commonly used by those with hearing impairment, is ‘lip reading’, which interprets movements of tongue, teeth and lips that signal the production of speech sounds that are frequently masked by background noise. Even here, the talker can influence the success of this method by ensuring that their mouth articulation is distinct as well as being visible to the listener.
We have measured the acoustic attenuation by three different types of face masks, as well as a face visor. We used four different face coverings:
- A cloth surgical mask where it was not possible to achieve a seal over the bridge of our synthetic nose.
- A fold-flat face mask rated at FFP3, the standard recommended for use with viruses. A bendable metal clip formed the mask shape around the bridge of the nose to form a good seal.
- A pre-formed face mask, also rated at FFP3, but using a foam band around the edge, sewn hinged to the inner face of the mask, to provide a good seal to nose and cheeks.
- A splash visor, as supplied to the NHS, which provides a full-length face covering to below the chin, but spaced from the forehead by a soft foam headband.
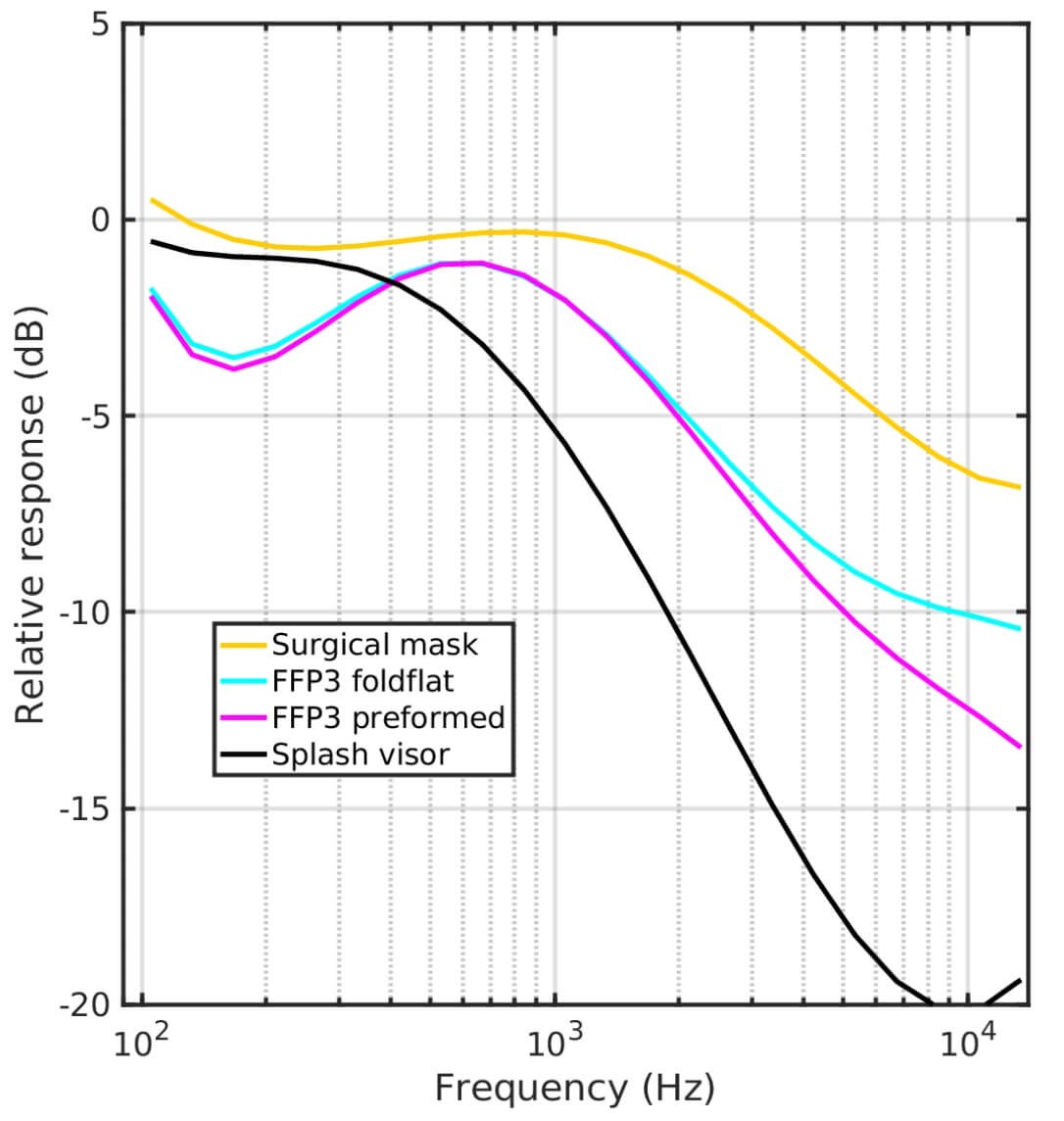
Figure 1. Smoothed attenuation characteristics measured on four types of face covering.
The smoothed attenuations are shown in Figure 1, plotted as dB as a function of frequency. They show that the surgical mask produced only a modest attenuation in most of the range of important speech frequencies, with a maximum of about 6 deciBel (dB), representing a quartering of the sound power delivered.
Both styles of FFP3 mask produced a very similar attenuation characteristic, doubling the attenuation compared to the surgical mask. The splash visor produced a much greater attenuation. All coverings produce attenuation in the frequency region above 1-2kHz.
Presbyacusis, age-related hearing loss, typically exhibits only a small loss at frequencies below 1kHz, but gradually increasing with frequency above 1kHz. Therefore, the general shape of these attenuation characteristics is likely to produce difficulties in the frequency range just where the hearing-impaired listener already has difficulties.
Hearing impairment is coarsely quantified into steps of normal, mild, moderate, moderate-severe, severe and profound, depending on the degree of measured hearing loss. An attenuation of 8-10dB would translate into an equivalent degradation of hearing by one of these steps. So even a person with ‘normal’ hearing would be at a disadvantage in communication.
Although Lazzarino [2] suggested that less clear speech would prompt reduced physical separation between talker and listener, in practice, for the attenuations reported here, the benefit would be small.
In many everyday situations, people with hearing impairment need to communicate in situations with background noise. A recent estimate of this reported that the speech level would only be 5dB higher than a background of babble noise, or 8dB higher than a background radio or television [3]. In these scenarios, the face covering would muffle the talker, making it harder to hear, because the background sounds themselves are not muffled by the mask.
We have therefore simulated the effects of listening to speech produced from under each of the above masks, with a background of either a babble of four talkers or a single talker. These each consist of seven seconds of the speech without the effect of the face covering, followed by the same seven seconds of speech but including the effect of the face covering.
Single talker against single competing talker such as radio:
tv_surgical+8dBSNR.wav
tv_FFP3foldflat+8dBSNR.wav
tv_FFP3preformed+8dBSNR.wav
tv_SplashVisor+8dBSNR.wav
Single talker against competing four-talker babble:
babble_surgical+5dBSNR.wav
babble_FFP3foldflat+5dBSNR.wav
babble_FFP3preformed+5dBSNR.wav
babble_SplashVisor+5dBSNR.wav
Conclusion
When wearing a face covering, a talker needs to take extra care in their speech production, even if the listener is presumed to have healthy hearing. ‘Extra care’ includes a range of factors detailed above, more than just raising the level of one’s voice.
References
1. Greenhalgh T, Schmid MB, Czypionka T, et al. Face masks for the public during the covid-10 crisis. BMJ 2020;369:m1435.
www.ncbi.nlm.nih.gov/pubmed/25690777
2. Lazzarino AI. Rapid response to BMJ 2020;369:m1435.
www.bmj.com/content/369/bmj.m1435
3. Smeds K, Wolters F, Rung M. Estimation of Signal-to-Noise Ratios in Realistic Sound Scenarios. J Am Acad Audiol. 2015;26(2):183-96.
www.bmj.com/content/369/bmj.m1435/rapid-responses





