Audiology has changed dramatically in recent years. Cochlear implants and high power hearing aids have made hearing really available to children with essentially any degree of hearing loss. Those of us who have been in the field for a long time remember how difficult it was to tell parents that their child had a severe to profound hearing loss before current technology was available.
We knew they could learn to talk but it was going to take a lot of work and their voices would always have that ‘deaf’ quality. Things have changed. I certainly am much more optimistic about opportunities for children with hearing loss than I was 20 years ago but now that technology is better, are we getting careless?
Responsibility of audiology
Yes, children with hearing loss are able to hear more with new technology, but that does not mean that life is easy for them, nor does it mean that our jobs are easy now. Fitting technology is only the beginning. The work may be easier now with current technology, but the work is not done. Audiologists have a critical role in managing hearing loss – one that no one else can do. Only audiologists are responsible for being certain that kids are hearing well enough to use hearing to develop the auditory brain and to learn language. This can only be accomplished by testing. We cannot assume. Real Ear testing will tell us what is reaching the tympanic membrane but not what is reaching the brain. Without testing we are guessing at how a child is hearing. Verification requires testing thresholds with technology and testing speech perception at normal and soft conversational levels in quiet and in background noise.
“Audiologists have a critical role in managing hearing loss – one that no one else can do. Only audiologists are responsible for being certain that kids are hearing well enough to use hearing to develop the auditory brain and to learn language.”
What should we expect?
With the technology we have available today we should expect children to be able to hear at or near the top of the speech banana – in the area I call the ‘speech string bean’.
Hearing at the level of the speech string bean will allow the child to hear normal and soft speech. If a child is not hearing at a sufficiently soft level they may not be able to hear soft speech. Soft speech permits a child to ‘overhear’ conversation and ‘overhearing’ accounts for more than 50% of what a child knows [1]. Soft speech is at 30-35BHL. If a child does not hear comfortably at that level he will not be able to overhear speech which will affect language and literacy.
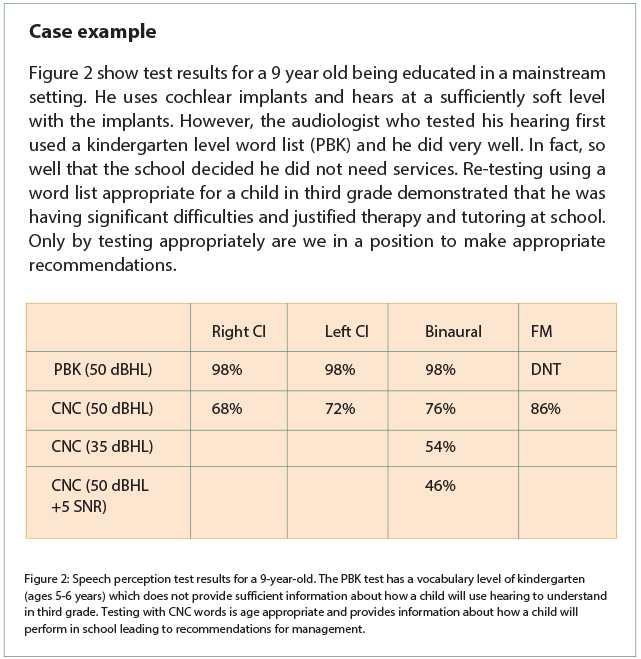
Aided thresholds do not tell us how well a child understands speech, or whether the signal is distorted. Speech perception needs to be tested using age appropriate tests, and at normal and soft levels in quiet and in competing noise to be certain we know what a child hears.
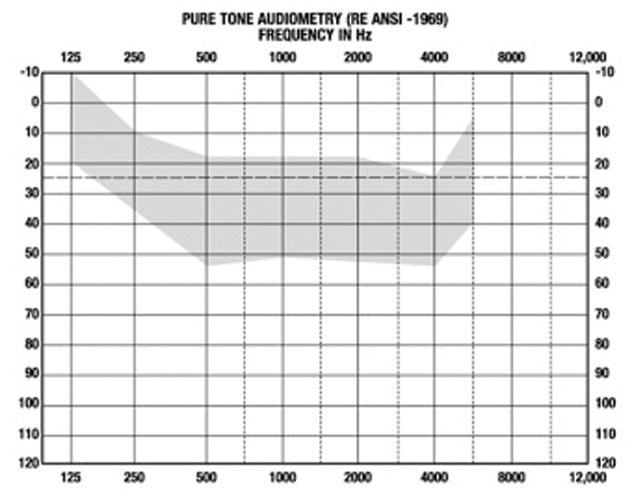
Figure 1: Speech banana with speech string bean identified. The string bean is the goal.
Using test results
By carefully reviewing test results we can determine both how a child is performing and what the child needs. And, yes, it is the responsibility of the audiologist to determine what the child needs. Audiologists see children less often then the teachers, therapists or parents who work with the child so audiologists have the opportunity to monitor progress in a different way.
By reviewing audiologic test results we can determine if a child is hearing softly enough. If she is not, it is the responsibility of the audiologist to change technology settings to provide access at the level of the string bean. If hearing aids cannot be adjusted to provide sufficient access, the audiologist is the person who can refer a child for consideration of a cochlear implant.
By reviewing speech perception test results, the audiologist can determine if a child understands speech clearly [2]. If a child has poor speech perception at normal conversational levels we know he will have difficulty learning using audition alone and will require auditory based therapy to build skills. If a child cannot hear soft speech clearly, it will be essential to recommend an FM system for use at home and at school. If a child cannot hear and understand speech in noise, an FM system should be recommended for all difficult listening situations, including sports and other after school activities.
If a child is hearing at the level of the speech string bean but cannot understand speech, the audiologist has to determine if there is distortion in the technology or if the problem is a therapy one. If a child hears sufficiently softly and still does not understand it is essential to determine why. Has the child not received sufficient auditory based therapy? Does the child have other learning issues that need to be addressed? The audiologist is the person who needs to monitor and manage audition. Even if audiologists cannot control therapy and school services, they have the responsibility to discuss concerns with families, therapists and schools.
Conclusion
Paediatric audiology is an exciting and complicated profession. Audiologists should not be limiting what they do to testing hearing and fitting hearing aids using Real Ear measures. Those limitations are both unrewarding, and, more importantly, not providing children with hearing loss with all the help they need to be the best they can be.
References
1. Akhtar N, Jipson J & Callanan MA. Learning words through overhearing. Child Development 2001;72(2):416-30.
2. Madell JR. (2014) Evaluating Speech Perception in Infants and Children. Pediatric Audiology: Diagnosis, Technology and Management, 2nd edition. New York USA; Thieme; 103-20.
Declaration of Competing Interests: None declared.


