Introduction
When perceiving sounds in real-world listening environments, older adults encounter several sources of degradation that can interfere with the perceptual process (Figure 1). Target signals (i.e. the sounds that a listener wants to focus on) have specific acoustic characteristics (e.g. spectral shape and changes in spectrum over time) that the auditory system must encode and resolve. These physical cues may be altered due to the presence of competing sounds or reverberation in the environment.
If the older listener wears hearing aids, digital signal processing algorithms in the amplification device, which are designed to improve perception by listeners with hearing loss, may generate unwanted distortion along with desired signal modifications. Older listeners may also encounter additional target-signal degradations due to the presence of cochlear hearing loss and age-related changes in higher-level processing.

Figure 1: Factors that may contribute to signal degradation by older adults with hearing loss.
For example, cochlear hearing loss makes sounds harder to detect due to reduced audibility, but the loss may also cause degradations in the analysis of the spectral and temporal properties of the target signal. Processing that occurs ‘upstream’ from the cochlea may also impact the older adult. Listeners with fewer cognitive processing resources may have more difficulty making use of ‘top down’ processing when decoding the degraded input coming from the auditory periphery.
Our research seeks to characterise the individual and combined effects of these different forms of degradation on speech perception in older adults. We are interested in two related questions. Firstly, how much of the loss of intelligibility and reduction in signal quality is due to the peripheral hearing loss? And secondly, once the peripheral effects are accounted for, what remaining factors contribute to the variability in how older adults respond to signal degradations? That is, why are some older adults more susceptible to signal distortions even when the peripheral losses are similar?
An important tool in our research is the use of objective metrics which allow us to quantify the cumulative effects of signal degradations caused by noise, hearing aid signal processing and peripheral hearing loss. In this review, we first describe how our metrics quantify signal degradations and then discuss two general ways we have used these metrics in studying hearing and cognition in older adults.
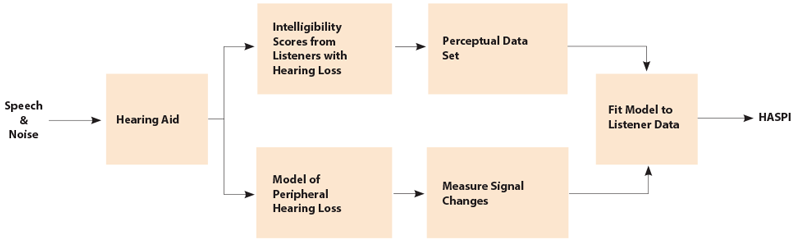
Figure 2: Overview of the Hearing Aid Speech Perception Index, an objective metric of speech intelligibility.
Objective metrics
We have developed metrics both for speech intelligibility, the Hearing Aid Speech Perception Index (HASPI) [1], and for sound quality, the Hearing Aid Speech Quality Index (HASQI) [2]. Both of these metrics are based on measuring changes in the signal at the output of a model of the auditory periphery, and then developing mathematical models that match the measured signal changes to the listeners’ intelligibility scores or quality ratings. This approach is illustrated in Figure 2 for HASPI. Listeners are asked to identify words in a set of sentences where the speech has been degraded by noise and by the distortion produced by the hearing-aid processing. The intelligibility scores form a perceptual data set indicating how the different forms and amounts of degradation affect speech intelligibility. Each of the degraded sentences is also passed through a model of the impaired auditory periphery to produce auditory signals for each combination of processing condition and hearing loss.
These signals are compared to the outputs for the noise-free undistorted speech passed through a model of normal hearing. The signal changes are quantified and combined to give a prediction of speech intelligibility, with the parameters adjusted to minimise the error computed over intelligibility experiments evaluating a wide range of processing conditions including noise, nonlinear distortion, dynamic-range compression, and frequency compression. A similar procedure is used for HASQI to relate the measured signal changes to listener quality ratings; however, for HASQI the noise-free reference signal is passed through a model of the impaired periphery rather than a model of normal hearing.
The auditory model used for the metrics reproduces important aspects of normal and impaired hearing. The model starts with the middle ear, followed by a filter bank that reproduces auditory frequency analysis. The filter bandwidths are adjusted to give the increase in bandwidth associated with increasing hearing loss. The dynamic-range compression mediated by the outer hair-cell behaviour is incorporated into the model, with the model reducing the amount of compression with increasing loss. Two-tone suppression is also present in the model, with the amount of suppression reduced with increasing loss. Inner hair-cell damage is present as a threshold shift added to the threshold shift associated with the outer hair-cell damage. The outputs of the auditory model are the modified signals in each frequency band, along with the signal envelopes. Intelligibility and quality are related to the fidelity in reproducing the variations in spectral shape over time and to the accuracy in reproducing the temporal fine structure within each frequency band.
The metrics provide a mathematical relationship between the extracted signal characteristics and the listener intelligibility scores and quality judgments. The indices produce a value ranging from 0 to 1, with 0 indicating poor intelligibility (HASPI) or poor quality (HASQI) and 1 indicating perfect intelligibility or quality that is indistinguishable from a perfect reference signal. Given a large set of signal manipulations and associated judgments, the indices provide a summary of how signal changes impact sound quality, that is, a distillation of the experimental evidence into a single compact representation. The indices provide data fits averaged over subjects; the impact of changes to the auditory periphery is included in the models, but the effects of individual cognitive differences have been removed by the averaging.
Using metrics to learn about cognition and hearing The metrics are a valuable tool in our research on the role of cognitive factors in older listeners’ response to hearing aid signal processing. The index measurements can be used in two ways: they indicate the physical changes in the signals caused by the processing used in the experiments and they can also be used to estimate the impact of the peripheral loss on the subsequent intelligibility and quality judgments. In some of our recent work, we use the metrics to quantify the cumulative degradation caused by noise and hearing aid signal processing. We then consider whether listeners with particular patient characteristics (e.g. poor working memory) respond to specific amounts of distortion differently than other patients.
Our results are consistent with the idea that when listening to noisy speech, older adults with hearing loss and with poor working memory are especially susceptible to distortions caused by hearing aid signal processing [3]. In our studies of hearing and cognition, we also leverage the fact that the metrics are highly effective in predicting average response to signal degradation [2]. The extent to which listeners differ from this average provide insight into whether individual listeners are more or less susceptible to distortion. We can then consider other factors (such as working memory) that might explain this increased susceptibility. One approach is to determine how much of the variance in the listeners’ responses can be explained by the metric predictions, which are based on the signal processing and the audiograms. The remaining variance can then be assumed to be related to causes beyond the periphery, such as working memory or executive function [4].
Acknowledgements
Work funded by National Institutes of Health R01 DC012289 and by a research grant to University of Colorado from GN ReSound.
References
1. Kates JM, Arehart KH. The hearing aid speech perception index (HASPI). Submitted for publication 2014.
2. Kates JM, Arehart KH. The Hearing-Aid Speech Quality Index (HASQI) Version 2. J Audio Eng Soc 2014;62:99-117.
3. Arehart KH, Souza PE, Baca R, Kates JM. Working memory, age, and hearing loss: susceptibility to hearing aid distortion. Ear Hear 2013;34(3):251-60.
4. Kates JM, Arehart KH, Souza PE. Integrating cognitive and peripheral factors in predicting hearing-aid processing benefit. J Acoust Soc Am 2013;134(6):4458-69.
Declaration of Competing Interests: JK retired from hearing aid manufacturer GN ReSound in September 2012. His research at the University of Colorado is currently funded by a research grant from GN ReSound.




