The hearing device landscape is rapidly changing, and what should be given, to whom, and why, are questions that many hearing healthcare professionals are asking. Brent Edwards discusses these questions and how consumer characteristics may influence their choice.
In 2016, President Trump signed a bill that requires the FDA to create an over-the-counter (OTC) category of hearing aid [1]. This new category of hearing aid is intended for use by adults with perceived mild to moderate hearing loss to be used and fit without the involvement of a licensed professional. This comes at a time when hearing aids and consumer electronics products are converging in technology and features.
A category of hearing devices called ‘hearables’ is also emerging; these are ear-level devices that provide audio and have wireless capabilities but are not intended to compensate for hearing loss. These consumer electronics products have many features that exist in hearing aids, such as directional microphones, while hearing aids fit by hearing care professionals (HCPs) are starting to have features typically found in consumer electronics such as step-counting. Meanwhile, even before OTC hearing aids become available, FDA-regulated hearing aids sold over the internet are becoming more common. This rapidly changing marketplace of hearing devices is causing confusion among healthcare professionals and consumers when determining the differences between HCP-fit hearing aids, OTC hearing aids, and hearables and what role these products will have in an HCP’s practice in the future.
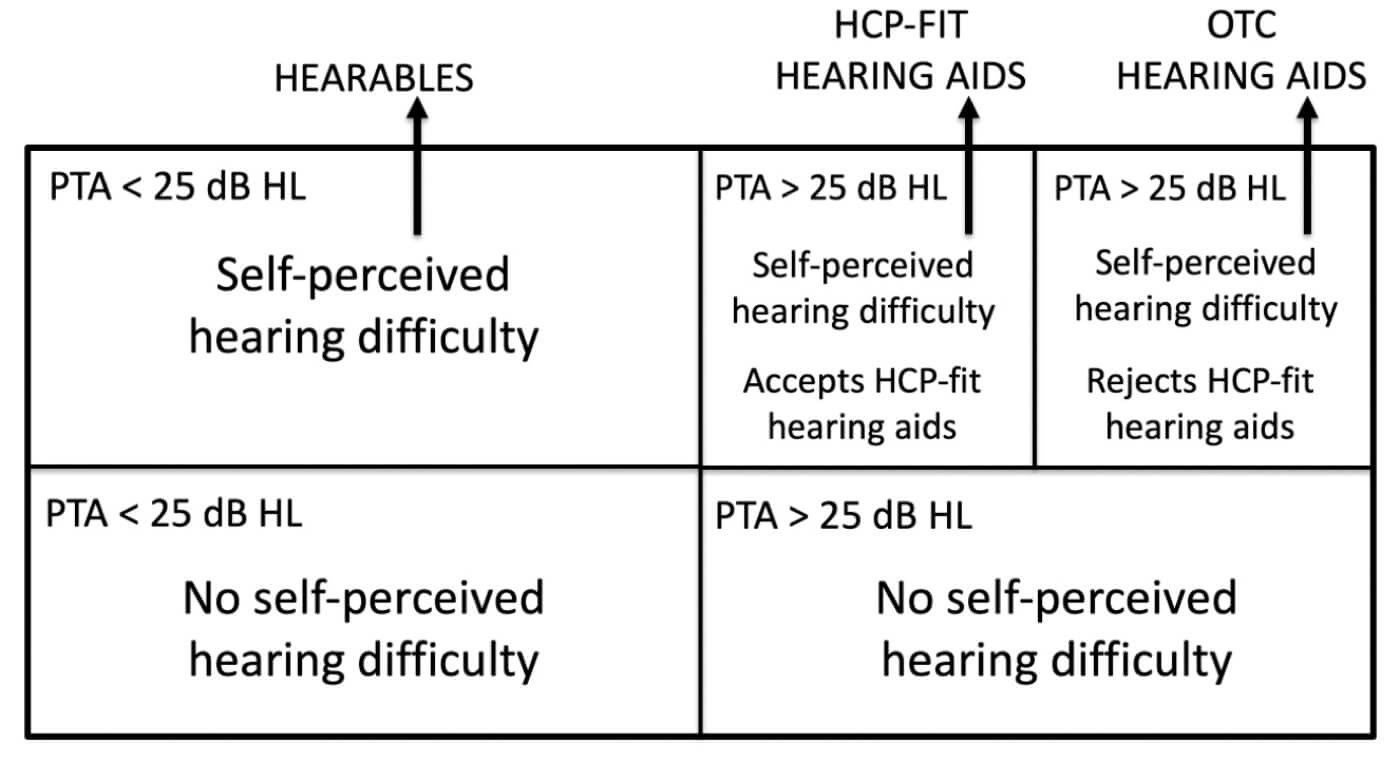
Figure 1. Segmentation of the population of people with auditory dysfunction. A PTA>25dB HL indicates audiometric hearing loss. Population segments optimal for hearable devices, hearing care professional (HCP)-fit hearing aids, and OTC hearing aids are noted with arrows.
Who are they for?
Whether a product is an HCP-fit hearing aid, an OTC hearing aid or a hearable depends on the intended use of the device and for which group of people it is designed. Figure 1 shows a segmentation of the population of people with auditory dysfunction that can help understand which products are for which population segment. In this figure, people with auditory dysfunction are categorised by whether they perceive themselves as having hearing difficulty, whether they have a measurable audiometric hearing loss as determined by the audiogram and, of those with an audiometric hearing loss, whether they accept an HCP-fit hearing aid as a solution.
Those with no self-perceived hearing difficulty will not be candidates for any hearing treatment since they have no perceived need for hearing help. Those with no audiometric hearing loss but self-assess as having hearing difficulty are candidates for hearables. Beck et al [2] estimated this population size in the US to be 26 million adults.

Of the two segments who have audiometric hearing loss and perceive themselves as having hearing difficulty, a significant portion of them have accepted an HCP-fit hearing aid as a solution and have been fit with hearing aids. Those who, for whatever reason, have not accepted HCP-fit hearing aids as a solution still have a self-perceived need for hearing help, and OTC hearing aids may be a solution for them since affordability and accessibility are two reasons that people in this group do not have hearing aids - issues that OTC is intended to address. Note that while the total population with an audiometric hearing loss in at least one ear has been estimated in the US to be 47.3 million (and 29.9 million for those with bilateral audiometric hearing loss) [3], not everyone in this group has a self-perceived need for help and therefore the size of the population who are actual candidates for HCP-fit or OTC hearing aids is smaller than those numbers cited [4].
In summary, the differences between hearables, HCP-fit hearing aids and OTC hearing aids will depend on which consumer segment they address rather than specific differences in technology.
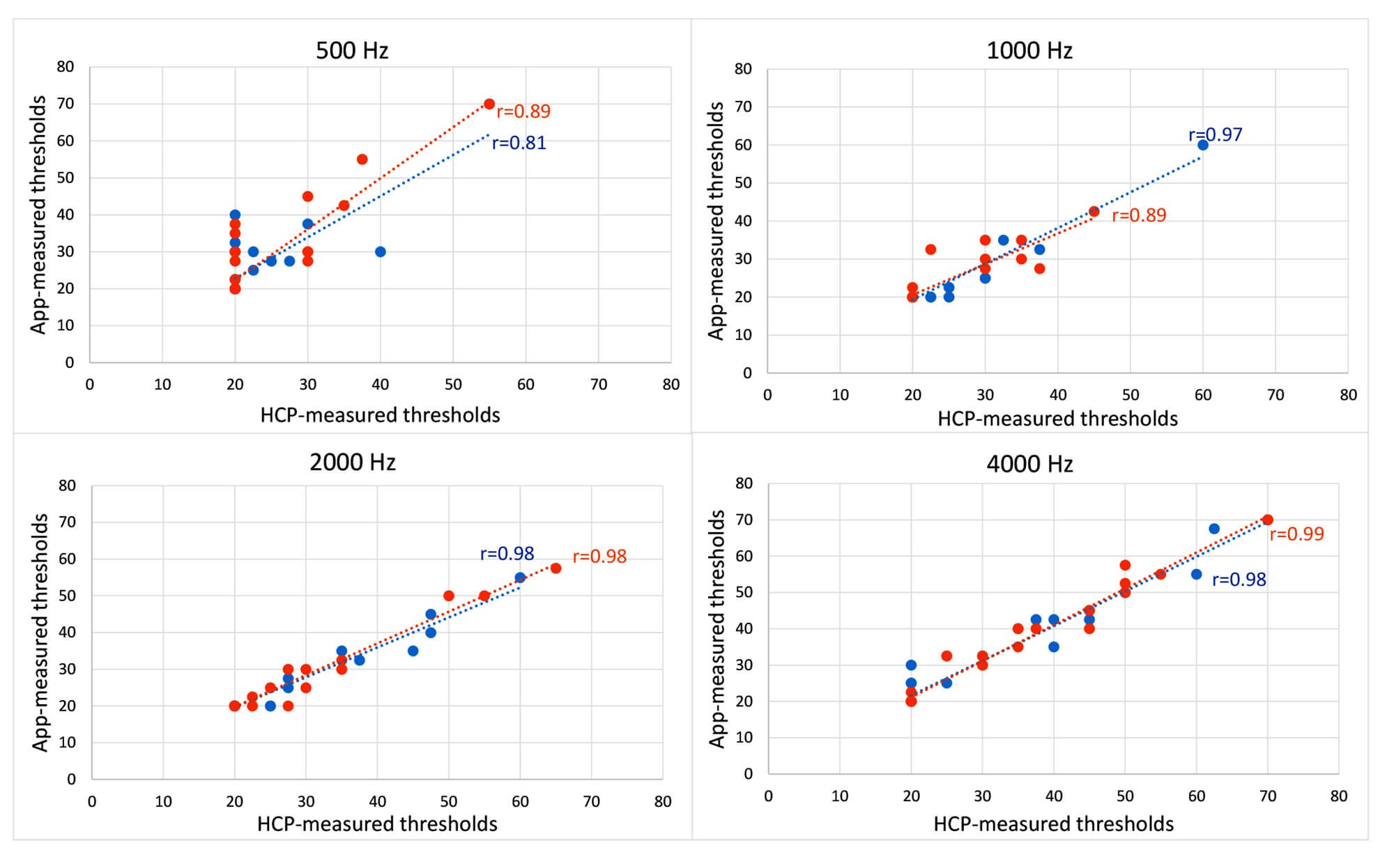
Figure 2. Comparison of the accuracy of an HCP-administered audiogram and self-assessed hearing thresholds using a smartphone app for frequencies 500, 1000, 2000 and 4000 Hz. Pearson correlation coefficients are given within each figure. Data are for left ear (blue circles) and right ear (right circles).
Self-fitting
One of the requirements of the OTC hearing aid bill is that users be able to customise the hearing aids themselves. There are several ways that this could be implemented, including methods that allow the user to measure their own pure-tone hearing thresholds and then automatically set the gain and other features based on the threshold results. Several smartphone apps exist today that allow for self-threshold testing. The National Acoustic Laboratories assessed one app that allowed the user to measure their thresholds at 0.5, 1, 2 and 4kHz. We compared thresholds measured by a user with a smartphone app in a quiet room to those measured by an audiologist in a sound-proof booth using standard clinical procedures: 15 people with normal audiometric hearing and 15 people with hearing loss were tested. The results, shown in Figure 2, show that the self-assessment method was highly consistent with the clinical measures. The correlation between the two was lowest at 500Hz, presumably because of interference with room noise at that frequency for the self-assessment data.
Other innovative methods have been developed that can successfully allow users to self-fit their hearing aids without requiring the measurement of an audiogram. Thus, there are no technical limitations in the fitting of OTC hearing aids, although there might be limitations in the ability of the user to administer the self-fitting technology.
OTC challenges
One of the challenges that OTC hearing aids face is getting the purchaser of these devices to be a successful user. HCPs spend many hours with their client getting them used to their devices: making adjustments to the hearing aid sounds processing based on complaints of the wearer, counselling the client on how to manage their hearing loss, motivating them to use their hearing aids, and training them on the care and use of their hearing aids. None of this professional help will be available for the OTC hearing aid user.
Convery et al [5] tested how successful people are with simply getting to a successful start with a hearing aid designed to be self-fit. They found that only 25% were successful on their own, 43% were successful if they received help from a trained assistant, and 32% simply could not get to a successful start even with help from a trained assistant. Some of the factors that predicted success were user self-efficacy and locus of control, suggesting that characteristics of the user will play an important part of whether someone will be successful with an OTC hearing aid.
For people who are current wearers of HCP-fit hearing aids, their level of satisfaction with their HCP is typically very high. Post-fit outcome data also suggests that the level of satisfaction and success with their hearing aids is dependent on the level of care that they received from the HCP. Thus, the need for an HCP is unlikely to go away with the introduction of OTC hearing aids. Given that hearing loss is a healthcare issue, many people are still going to want to see a healthcare professional for help. The presence of OTC reading glasses, for example, has not kept people from seeing optometrists to get their vision tested.
“The differences between hearables, HCP-fit hearing aids and OTC hearing aids will depend on which consumer segment they address rather than specific differences in technology”
Conclusion
What is likely to happen with the introduction of OTC hearing aids is that a new segment of people with audiometric hearing loss who are currently rejecting help from an HCP will be able to get help on their own. Many of these people will not be successful with their OTC hearing aids either because of deficiencies with the product or due to their own needs for professional help. Other people will not be interested in OTC products and choose to see an HCP, particularly if their perceived hearing difficulty is significant or they believe that they need an expert in hearing healthcare to assess and treat their hearing. The development of connected hearing healthcare will provide many new methods for the provision of this healthcare, eliminating some of the need for face-to-face appointments.
References
1. Warren E, Grassley C. Over-the-Counter Hearing Aids: The Path Forward. JAMA Intern Med 2017;177(5):609-10.
2. Beck DL, Danhauer JL, Abrams HB, Atcherson SR, Brown DK, Chasin M, Clark JG, De Placido C, Edwards B, Fabry DA, Flexer C, Fligor B, Frazer G, Galster JA, Gifford L, Johnson CE, Madell J, Moore DR, Roeser RJ, Saunders GH, Searchfield GD, Spankovich C, Valente M, Wolfe J. Audiologic considerations for people with normal hearing sensitivity yet hearing difficulty and/or speech-in-noise problems. Hearing Review 2018;25(10)[Oct]:28-38.
3. Lin FR, Niparko JK, Ferrucci L. Hearing loss prevalence in the United States Archives of internal medicine 2011;171(20):1851-2.
4. Edwards B. What outsiders tell us about the hearing industry. Hearing Review. 2006;13(3):88-92.
5. Convery E, Keidser G, Hickson L, Meyer C. Factors Associated With Successful Setup of a Self-Fitting Hearing Aid and the Need for Personalized Support. Ear and hearing 2019;40(4):794-804.
Declaration of Competing Interests: The National Acoustic Laboratories (NAL) received devices and financial reimbursement from Nuheara for the study comparing the threshold measurement performance of the Nuheara app to an audiologist-measured audiogram. The study was independently conducted by NAL and was approved by the Australian Hearing Huma Research Ethics Committee.
Acknowledgements
The author would like to thank Elizabeth Beach, Jermy Pang and Lyndal Carter for the work comparing app-measured thresholds to audiologist-measured thresholds, and Nuheara for providing devices and funding for the data gathering.