In January, we first heard of COVID-19. As we currently do battle with it on our own shores, colleagues in China share their story with us as life there slowly and cautiously begins to return to normal and the country appears to be on the long road to recovery. Dr. Jiao Xia and Prof Shusheng Gong of the Beijing Friendship Hospital recount their experience of the pandemic, and what it meant for the ENT profession in Beijing.
It all started with a request to attend an emergency department meeting on 21 January 2020. There was a report of a new respiratory infectious disease which was spreading quickly in Wuhan. The department was urged to build an emergency response team in case the situation worsened. After two days, the Wuhan government announced the shutdown of the city due to the widespread outbreak of COVID-19, the illness caused by the coronavirus. The next day, Beijing launched the first-level response for a major public health emergency and across China, all 31 provinces and municipalities took serious measures. On 12 March, WHO declared the COVID-19 pandemic, which has caused more than two million confirmed cases and more than 147,000 deaths as of 17 April 2020.
Under the strong leadership of the Communist Party of China Central Committee with Comrade Xi Jinping at the core, Chinese people have united and taken the strictest measures to battle the epidemic. After more than two months’ national massive efforts, the Chinese have turned a corner in battling the disease. Here, we would like to present the real-life experiences of the common Chinese people and ENT colleagues during the outbreak.
How it changed our personal lives in Beijing
All citizens were required to have a temperature test before getting into the buildings or close communities in Beijing during the period of first-level response. The government called upon citizens to stay at home, wear masks when going out, wash hands frequently and undertake social distancing. The last time the same level of emergency response occurred in Beijing was during the SARS outbreak in 2003. This helped as most citizens understood what the first-level response meant. As it started in the week of Spring Festival holiday, most people had scheduled family dinners, parties or travels to celebrate Chinese New Year but citizens responded to the call voluntarily by stopping unnecessary travel. My parents and child have not left the community for more than two months. Thanks to the sophisticated and convenient delivery system, we did not experience panic buying for food or other household goods. Even during the festive time of national holiday, the markets are normally well-supplied in Beijing. People ordered food, household items, masks and sterilisation products online. The untouched delivery was suggested to protect both deliverers and customers. The schools were closed after the holidays and children did online classes for the last eight weeks. For some of the essential workers who had to go back to work, childcare became a challenge.
The decrease in social contact proved to be the critical factor in controlling communicable diseases in the Chinese experience. There was a significant impact in the catering industry and other service industries. Most restaurants and retail businesses turned to online sales to negate their losses. Some enterprises and public institutions gradually resumed work after 9 February in Beijing and, on government advice, this was done by working remotely and by staggered shifts. People used smartphone apps and were categorised by a Health QR code to indicate whether they are at risk of contracting the new coronavirus and needed to self-isolate. (see Figure 1).

Figure 1. Based on citizens’ health data, those with green Health Codes can go to work and travel freely, while the people with red codes are still in the period of quarantine and cannot get into public places.
Though there was no community transmission found in Beijing for several weeks, the city still faced the massive pressure of imported cases, so the government has not decreased the response level. Most citizens agree with it despite the inconvenience of daily life and the economic loss. Personally, I have spent more time with my family than ever during the past two months, and the inconvenience was quite acceptable for most.
How it changed the ENT professional in Beijing
Almost every secondary and tertiary hospital setup a fever clinic after the SARS outbreak in China. The fever clinic is open 24 hours as an emergency department but remains relatively independent to avoid cross-infection (see Figure 2). All fever patients would have a flu screening there before any specialist consultation. After the COVID-19 outbreak, the fever clinic was the frontline to screen patients and faced a huge workload. To overcome the staffing issues, all the departments in our hospital were redeployed to support on a formal rota. To prevent the infection spreading, the staff in the fever clinic needed to stay in the hospital for a two-week shift followed by two weeks’ self-isolation. Three doctors and four nurses from the ENT department worked in the local fever clinic at one time. In Beijing, all fever patients were screened in this clinic from January and the confirmed cases were sent to three infectious disease hospitals for treatment.

Figure 2. The fever clinic of Beijing Friendship Hospital is in a separate building with the independent consulting rooms, a laboratory for the flu screening test and CBC, an observation room, the isolation rooms and the separate CT room.
From the end of January, online continuing education offered all healthcare staff the up-to-date knowledge of COVID-19. Seven editions of clinical guidance of the epidemic prevention and control were updated in the past two months in China. The English version handbook of COVID-19 prevention and treatment was published online.
https://www.alibabacloud.com/zh/universal-service/pdf_reader?pdf=Handbook_of_COVID_19_Prevention_en_Mobile.pdf
Our department was dealing with emergency patients during the epidemic. The outpatient number was controlled to half of the normal. The elective operations and unnecessary endoscopic examinations were postponed until March. The Society of Otorhinolaryngology, Chinese Medical Association, published the protection suggestions for ENT staff on 2 February. We applied for PPE in our hospital following the suggestions. The staff used level II protection including disposable surgical cap, medical protective mask (N95/FFP2), disposable latex gloves and goggles in the outpatient clinic. The disposable medical protective uniform was used in endoscopic examination and biopsy. The patients were required to wear masks and keep at least one meter’s distance in the waiting area (see Figure 3).
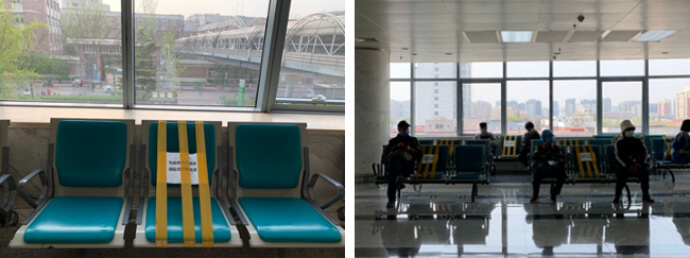

Fig 3. The hospital took measures to keep social distancing during the outbreak. The patients were required to wear masks and keep at least one meter’s distance during waiting. All patients received temperature test before getting into the consulting room.
Level III protection including disposable surgical cap, medical protective mask (N95/FFP2), disposable latex gloves and long barrel shoe cover as well as face respiratory protective devices or powered air-purifying respirators, were recommended for use when operating or intubating for the COVID-19 confirmed cases or suspected cases. Considering the false-negative possibility and time-consuming aspect of the Nucleic acid test and antibody test, we gave all acute cases complete blood count and chest CT scans before emergency surgeries. The typical multiple ground-glass opacity on CT and the low count of WBCs and lymphocytes indicate a high possibility of COVID-19. As things started improving in March, all patients were screened by taking CBC and chest CT scans on the day of hospitalisation. The patients with travel history or COVID-19 contact history were put on self-isolation for at least two weeks before hospitalisation. The bed utilisation rate was controlled at around 60%. Online consulting played an important role during the epidemic. Many specialists offered free online consultation to calm the anxious population and to help people who need a medical service out-with COVID-19 (see Figure 4).

Figure 4. Prof Shusheng Gong opened online consultation and gave lectures on social media and on TV to guide people on how to deal with ENT conditions during the epidemic.
The efforts of ENT specialists in Wuhan
Wuhan, the capital of Hubei province in central China and the epicentre of COVID-19, underwent migration control and mass quarantine for 47 days to localise the outbreak. We talked with Dr Yun Zhu, an ENT Consultant at Wuhan Union Hospital, about his experience during the past two months.
At the beginning of January, did you notice more patients come to ENT clinic because of fever, cough or throat pain?
Not really. Maybe because my hospital is a tertiary hospital and patients usually don't come to us directly. Also, the severe pneumonia patients are normally recommended to the respiratory medicine department.
When did you become aware of this infectious disease?
I heard about the unknown pneumonia spreading on a small scale connected to the Huanan Seafood Market at the end of December. I took it as an influenza-like disease first. At the beginning of January, we were warned by the Health Commission of Hubei Province to report the cases of pneumonia with unknown origin. After the pathogen was isolated and detected, it was confirmed to be a novel coronavirus. People started to connect it with SARS, and things got tense. Meanwhile, one patient had a fever after surgery in the ward of the neurosurgery department in my hospital, followed by one doctor and 13 nurses falling ill with a fever successively. The National Health Commission sent the High-level Expert Group to Wuhan urgently. The group leader, Academician Nanshan Zhong, declared the human to human transmission of novel coronavirus on 20 January.
How did the outbreak change your clinical practice?
The outbreak was before the two-week national holiday of the Spring Festival. We usually discharge all non-emergency patients during the holiday. With the extensive patient numbers, the senior ENT consultants took charge of all ENT emergencies, and the rest were called to join in the emergency, ICU and the mobile cabin hospital. I applied to work in the fever clinic and was in charge of the suspected or confirmed severe cases in the emergency observation room. Because the wards were full of patients during the first week of February, even severe patients had to stay there. Mild cases were encouraged to observe at home. Two new temporary hospitals and 13 mobile cabin hospitals opened within one week and the government carried out the new strategy that all confirmed patients should be isolated from family and treated in hospital. When I left the fever clinic in the third week of February, the pressure there had decreased remarkably. Thanks to the healthcare workers from other parts of China who came to support Wuhan, I took two weeks' break before I went to the buffering ward.

Dr Zhu and his colleagues were packing patients for transportation. Level III protection was used in emergency observation room where severe patients were treated before beds were released in ward.
What is the buffering ward?
When we came to March, all COVID-19 patients could be treated or observed in the corresponding hospitals according to the severity of symptoms. It was time to consider the other patients, such as patients with malignant tumours, cardiovascular accidents and other acute cases. They needed to be offered medical service in time and also to be protected from COVID-19.
Did you do tracheotomy for the COVID-19 patients? How did you protect the staff?
We did tracheotomies after one week of intubation. Level III protection, especially the powered air-purifying respirator, was used. The closed sputum suction system was needed. I haven't heard of any medical staff infected due to the operation or caring of tracheotomy if they used proper PPE.
We understood ENT to be the high-risk group for staff infection. What’s your opinion?
The staff of ENT, ophthalmology and oral medicine are at danger of exposure to patients’ secretions so during the outbreak, level II protection was necessary. With the proper PPE and following the standard procedure of donning and removing, we felt adequately protected. Most of the staff that were infected were exposed before the outbreak due to close contact with the patients without proper protection.
Thank you for your efforts in Wuhan. How is your family during the outbreak, and when will you go back to work in ENT?
Worried about infecting my family, I haven’t been home for almost two months. My parents helped me to take care of my child and thanks to the community volunteers, who sent food and essential items to my home during the lockdown of the city. The ENT department reopened on 16 March in my hospital. I will go back to ENT after one month of work in the buffering ward and another two weeks' isolation. I am looking forward to seeing my family and my colleagues before May.
By the end of March, more than 42,000 medical staff and professionals from the rest of China were working in Wuhan and other regions in Hubei. Sixty-one medical professionals sacrificed their lives in the fight against COVID-19 outbreak. The virus knows no national borders, and the epidemic distinguishes no races. It’s time for all to take the responsibility and China is helping other countries by sharing prevention and control experience, providing medical supplies, and cooperating on medical and scientific research. The traditional Chinese ‘tomb-sweeping’ day on 4 April, this year was observed as the national mourning day for the 3326 victims who died of the disease. May the deceased rest in peace and lives be aware that the battle is not over yet.



