Platelet-rich plasma (PRP) is being used in an increasing number of ENT conditions, with particular promise in the larynx.
Voice is a defining human characteristic. The ability to communicate with one another and to use the vocal folds (VFs) for other phonatory tasks, such as singing or laughter, has shaped our society and culture, regardless of where you live on the planet. In addition, nowadays more than a third of adults rely on their voice for their occupation.
Therefore, voice abnormalities have profound consequences. Anatomically, the VF has a unique architecture which is perfectly designed to meet its functional requirements of airway protection, airflow control and phonation, yet it is easily disrupted and not so easily restored.
As otolaryngologists, we are often faced with disease or damage to the VFs and can feel despondent over the limited options for how to address this. On a microscopic level, similar histological changes are seen in VF scar, atrophy and sulcus pathology, including a loss of hyaluronic acid, elastin and structurally mature collagen type III, which are replaced by more chaotic deposition of collagen type I. Inflammatory infiltrates may also be seen in chronic laryngitis. Stroboscopic findings can include loss of normal mucosal wave amplitude or excursion, incomplete glottal closure and poor synchronisation of vibration exacerbating contact issues. For me, one of the most daunting problems is trying to manage vocal fold scar. Diffuse fibrosis or direct injury that violates the lamina propria can render vibration impossible, with the resultant voice extremely difficult to produce and of poor quality.
"Most of the current therapeutic approaches are modestly successful at best and address a singular aspect of what is a complex dysfunction"
Effort and fatigue with phonation is a significant burden for the individual, and can result in occupational loss and reluctance to engage socially. Most of the current therapeutic approaches are modestly successful at best and address a singular aspect of what is a complex dysfunction. Remedies that increase glottic closure often do so at the expense of vibratory performance (as increased mass can impair oscillations). Those that try to improve vibration or release scar tissue are unpredictable and can engender additional damage to the delicate microstructure.
My doctoral research was undertaken in the study of VF scar, utilising an ovine model and testing a novel collagen type IA inhibitor that modulated SMAD3 – part of the TGF-β fibrotic pathway. Although effective, the drug I tested produced unwanted bleeding side effects and was not successfully brought to market (unsurprisingly!). However, in my mind, this cemented the idea that molecular manipulation of the fibrotic cascade was the optimal way to approach remodelling damaged VFs. Stem cell therapy and the rise of possible growth factor treatment was appealing but has remained inaccessible for most, as it requires access to a molecular lab to grow stem cells and produces only nanolitre quantities!
Serendipitously, one day in my office, I spotted my colleague, a rheumatologist, in the clinic room next door to me, walking around with vials of golden liquid. I then watched him inject one of his rheumatoid arthritis patient’s knees with this liquid, that I now know was platelet-rich plasma (PRP). As I looked at this golden liquid, the penny dropped. To be honest I wondered why I hadn’t thought of it long before. Plasma, enriched with anti-inflammatory cytokines and growth factors [1], loaded with platelets which are filled with more potent cytokine mediators (including PDGF, bFGF, VEGF, EGF, IGF, TGF-β)*, is simply produced in the office through a blood draw and spun for a mere 10 minutes in a centrifuge, allowing us to siphon off the golden liquor. In our chosen protocol, I draw two 8.5 ml acid citrate dextrose (ACD) vacutainers of whole blood and am rewarded with about 3.5–4 ml of PRP (by selecting the middle third of the plasma [1–3], containing the most platelets, above the buffy coat – Figure 1).
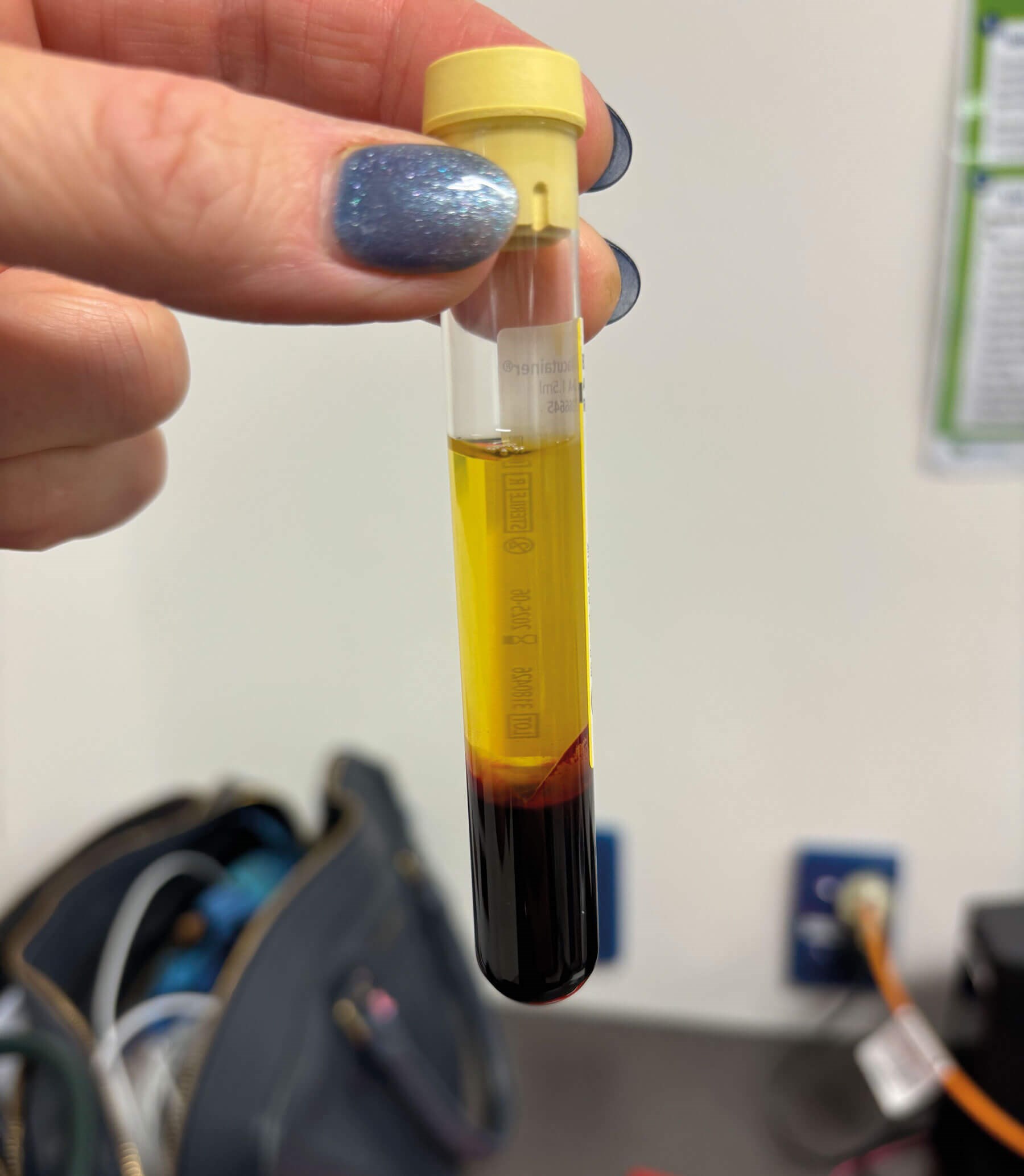
Figure 1: Photograph of acid-citrate-dextrose vacutainer tube after spinning whole blood in centrifuge, demonstrating the golden yellow plasma superiorly, a thin white layer (buffy coat) and the red cells inferiorly.
Then it is a simple task of reinjecting this (transcutaneously or transnasally) very superficially into the SLP envelope until the vocal folds are ‘kissing’ (Figure 2A & B).
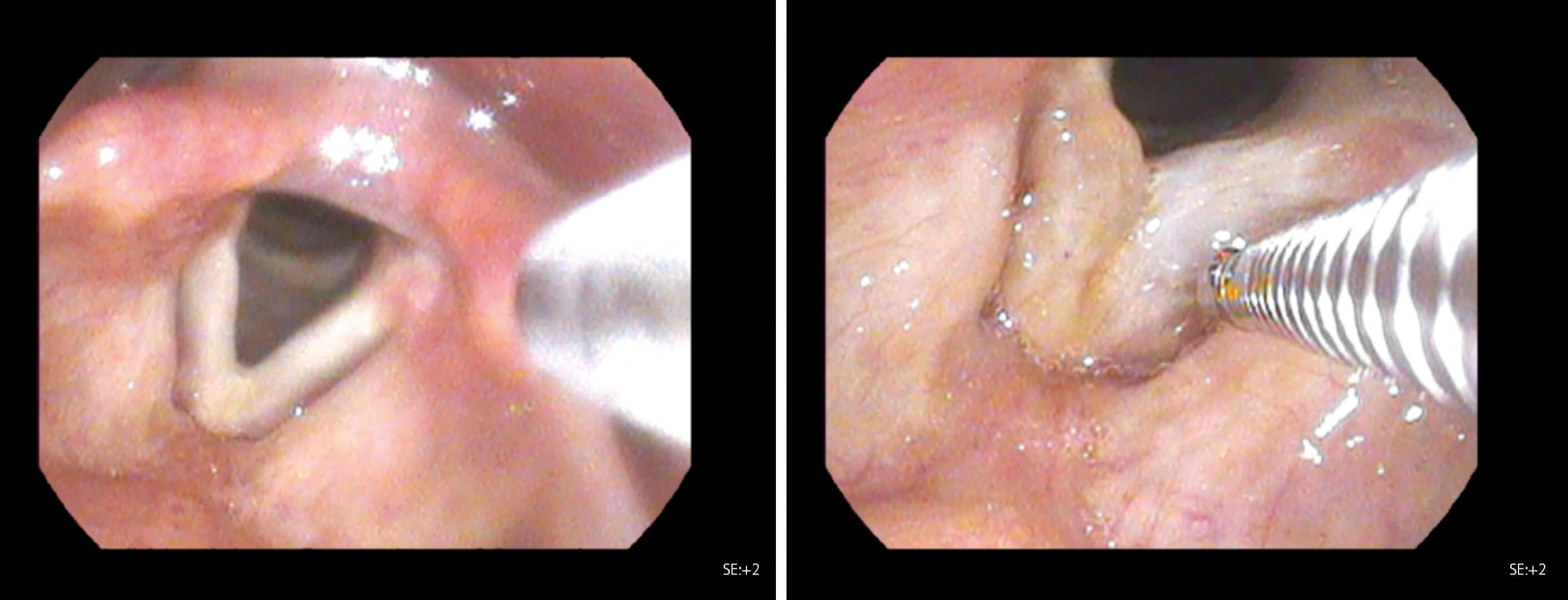
Figure 2: Endoscopic image of vocal folds before and after platelet-rich plasma injection. 2A shows vocal folds pre-injection, with tip of flexible needle sheath visible. 2B demonstrates post-injection appearance, with inflation of vocal folds and yellow discolouration from plasma.
The plasma has a water-like consistency and is rapidly absorbed by the body (within 6–8 hours). Over subsequent weeks, it induces remodelling of the vocal folds, increasing pliability and softening the tissue. This allows easier vibration at lower glottic airflow pressures, which patients perceive as reduced effort and improved voice quality. When there is less need to push or strain to achieve voicing, there is less fatigue and the voice can be used for longer, increasing functionality.
I tried this tentatively at first, in patients for whom I had exhausted other safe options for managing vocal issues. Following very positive early results, it became clear that this was a valuable treatment not only for patients with damaged folds, but also for those with minimal voice change, including vocal fatigue, unreliable voicing, voice deterioration during prolonged use, and age-related changes. These patients are often not quite affected enough to warrant traditional fillers, or fillers may risk worsening the voice by increasing the mass of the folds, compounding the sensation that phonation is effortful because greater airflow is required to achieve oscillation. PRP is the opposite. It addresses both a glottal closure issue and a vibratory issue in that it improves SLP pliability, allowing the same amount of air to create a greater excursion of the mucosal wave, and therefore achieving better glottal closure. The vocal folds remain the same mass, and pitch is maintained as normal. Initially, I postulated that due to the very small volumes injected, any positive benefits might be short-lived.
We have now been doing this for three years, in more than 150 patients, and around 50% of recipients have needed only a single dose. Those with greater damage to the vocal fold e.g. scar or previous procedures compared with atrophy are more likely to undergo additional injections [1]. If they do want another injection, it is a simple 30-minute procedure in the office, and we can readily accommodate their request.
"The appeal of PRP is enhanced by its safety (it comes from the patient and goes back into the patient), low cost, ease of preparation, speed of delivery and duration of benefit"
I have since used PRP in vocal complaints of presbyphonic voice, post-resection of VF lesions, post-radiation, chronic laryngitis, phonotraumatic lesions, glottal web and am using it universally in the operating room when I directly manipulate the VFs (e.g. laser or resection), to encourage better healing post surgery [1–3]. We have long-term follow-up data, (in some cases greater than 24 months) with validated scoring and patient-reported outcome measures showing continuing improvement as time goes by (improvement in VHI-10 >8 points) [1]. Most importantly for me, I have satisfied patients, including professional and elite voice users, with whom I am generally very cautious.
The appeal of PRP is enhanced by its safety (it comes from the patient and goes back into the patient), low cost, ease of preparation, speed of delivery and duration of benefit, all of which assist a publicly-funded but resource-poor health system. Patients are reassured by it being autologous and it seems effective on both new and established scar. In most cases, there is little risk in offering PRP, aside from the patient having to undergo the procedure.
It is not often that a sea change in your practice occurs once you are a consultant, but this has truly changed how I treat my patients. So, perhaps for me, PRP really has been liquid gold.
References
1. Mackay G, Allen J. Platelet rich plasma in the larynx. Curr Opin Otolaryngol Head Neck Surg 2024;32(6):374–82.
2. Mackay G, Prigent C, Allen J. Single platelet rich plasma glottic injections in vocal pathology demonstrate long term benefits. Laryngoscope 2026;136(2):847–53.
3. Mackay G, Allen J. Platelet rich plasma injection of the vocal folds in benign vocal pathologies. Eur Arch Oto Rhino Laryngol 2024;281:5419–28.
*PDGF – platelet-derived growth factor
bFGF – basic fibroblast growth factor
VEGF – vascular endothelial growth factor
EGF – epidermal growth factor
IGF – Insulin-like growth factor
TGF-β – transforming growth factor beta
Declaration of competing interests: None declared.
Jacqui Allen will be presenting on this topic at IFOS ISTANBUL 2026 in September.
Click here for more information.







