ENT surgeons may feel that they are the first point of referral for the majority of patients with snoring and possible obstructive sleep apnoea, but in reality a significant number of patients with sleep-disordered breathing (of any cause) are seen by respiratory physicians within dedicated sleep clinics. Rex Muza runs a tertiary referral sleep centre in London; in this article we hear about the patients he sees within that setting and the non-surgical treatment options available to them.
Sleep medicine is still very much an emerging and multifaceted discipline. Respiratory physicians, neurologists, psychiatrists and ear nose and throat specialists are some of the professionals who are involved in sleep research and sleep clinical practice.
There has been a recent increased awareness of the importance of sleep medicine which has led to an increased amount of referrals to sleep clinics. The obesity epidemic of our time with its resultant sleep-disordered breathing has thrust the respiratory physician to the forefront of sleep medicine.
“The obesity epidemic of our time with its resultant sleep-disordered breathing has thrust the respiratory physician to the forefront of sleep medicine.”
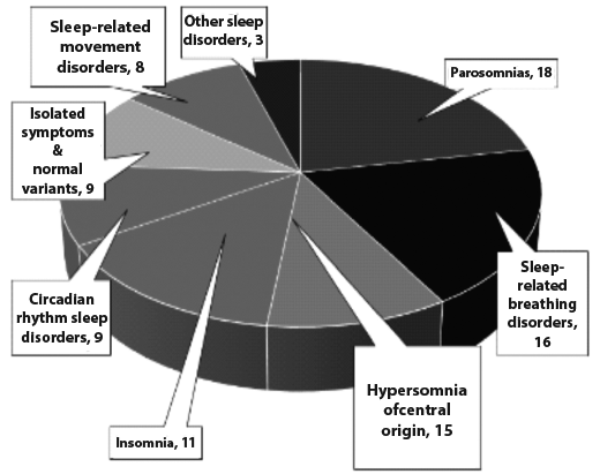
Figure 1: ICSD2 – 89 sleep disorders.
The International Classification of Sleep Disorders 2 (ICSD2) listed 89 sleep disorders [1]. Sleep-related breathing disorders accounted for 18 of those disorders (Figure 1). It is estimated that at least 2-4% of the adult population experience breathing-related sleep disorders. The mildest form of sleep-related breathing disorder is intermittent snoring, which is fairly universal without significant health sequel. The most severe forms of sleep-related breathing disorders are severe obstructive sleep apnoea and the obesity-hypoventilation syndrome, which are associated with severe morbidity and significant mortality. In between these two extremes are disorders of gradually increasing impact on morbidity and mortality: persistent-snoring, upper airway resistance syndrome and obstructive sleep apnoea hypopnoea syndrome.
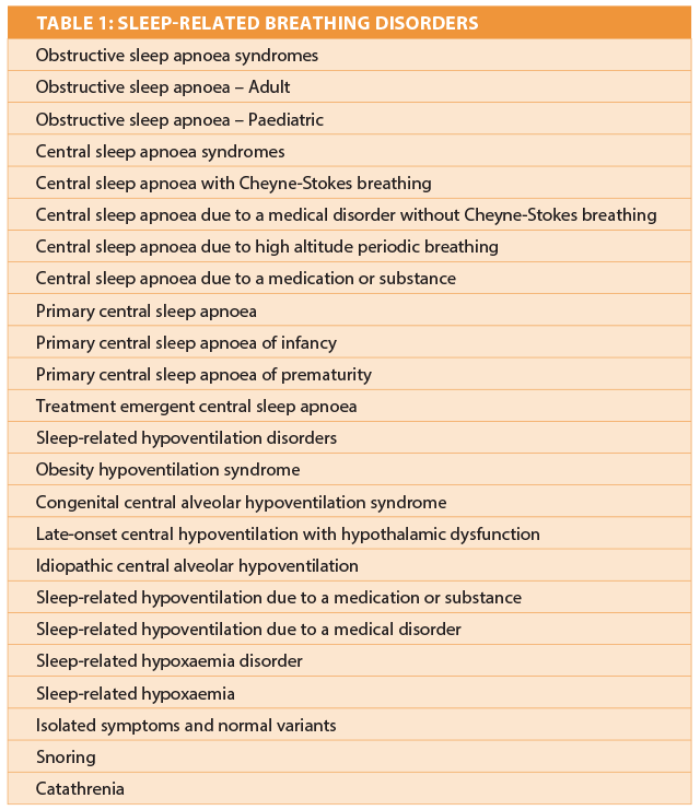
Table 1 lists the variety of sleep-related breathing disorders a respiratory physician might encounter. About 60% of referrals to sleep centres are for sleep-related breathing problems. Screening tools for obstructive sleep apnoea such as the STOPBANG (Snoring? Tired? Observed to stop breathing? High blood Pressure? Body mass index more than 35? Age over 50? Neck size large? Gender male?) have helped push up referrals to sleep clinics. In countries like the United Kingdom there has been a huge rise in sleep clinic referral with the majority of the referrals being for screening and treatment of sleep apnoea syndromes. This burden falls on the shoulders of a respiratory sleep physician. A two night home oximetry is the usual initial screening tool (Figure 2). One tertiary sleep referral centre in London screens about 3000 patients a year for possible obstructive sleep apnoea. Of these about 1000 per year are commenced on continuous positive airway pressure (CPAP) treatment. The same centre performs just over 2000 overnight in-house polysomnography studies per year with about a third of them being for sleep-related breathing disorders. Figure 2 shows the types of problems investigated by polysomnography over a six month period at the same London sleep centre.
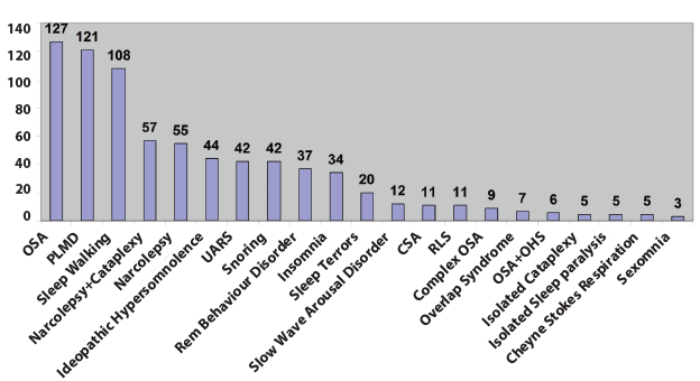
Figure 2: Breakdown of conditions studied by polysomnography at a tertiary sleep centre over a six month period.
A variety of non-invasive ventilation methods are available to help treat some of the sleep-related disorders respiratory physicians might encounter:
- CPAP devices provide continuous positive pressure in the airways thereby preventing them from collapsing and causing apnoea.
- Bi-level ventilator support has two levels of pressure, one on inhalation and one on expiration.
- An adaptive servo ventilator is a self-regulating ventilator for treating periodic nocturnal breathing conditions such as occurs in central sleep apnoea with the Cheyne-Stokes breathing pattern.
The respiratory physician is responsible for oximetry reporting and advising on the treatment options which may include simple oral appliances or commonly CPAP. Appropriately selected patients are referred for possible surgical interventions. The respiratory physician supervises the initiation of positive airway pressure (PAP) therapy. When stability has been achieved patients will usually have annual PAP technician follow-up only. Selected patients will have multichannel polysomnography depending on the type of the suspected sleep disordered breathing. Nocturnal hypoventilation syndromes will require bi-level ventilator support. Central sleep apnoea syndromes such as the Cheyne-Stokes breathing type, which is fairly common in patients with heart failure, may require special ventilation modes such as bi-level with a backup rate or adaptive servo ventilation. Again the respiratory physician, working together with cardiologists, sees to most of these patients.
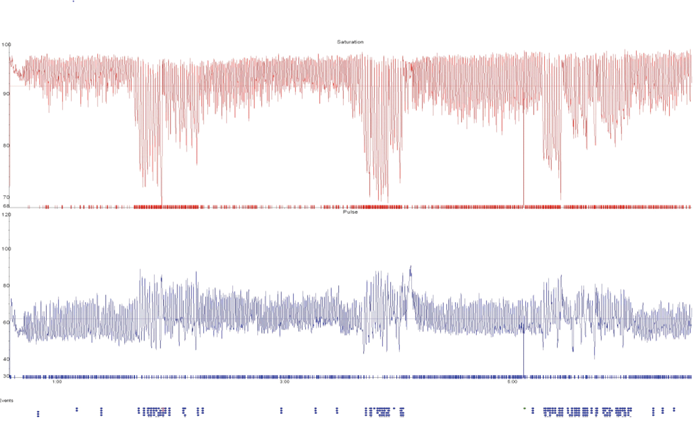
Patient A.
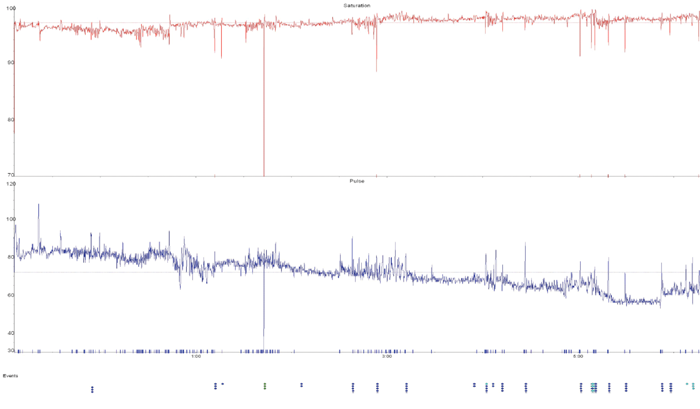
Patient B.
Figure 3: Oximetries of a patient with snoring but no significant obstructive sleep apnoea (A) and a patient with severe obstructive sleep apnoea (B) showing rapid deep desaturations (in red) with associated heart rate variability (in blue).
A number of respiratory conditions have symptoms which might worsen at night such as asthma. Patients with chronic obstructive pulmonary disease (COPD), neuromuscular disease and chest wall disease might need ventilator support in their sleep. Most respiratory physicians have a broad understanding of other sleep disorders and can manage a variety of the sleep disorders encountered in a sleep clinic.
Unfortunately there is still a huge unmet need of diagnosing and treating patients with sleep-disordered breathing. The Wisconsin sleep cohort study of patients estimated that 93% of women and 82% of men with moderate-to-severe sleep apnoea were undiagnosed [2]. The challenge is to further increase awareness, improve diagnostic rates and improve treatment methods.
References
1. The International Classification of Sleep Disorders. Second edition. Diagnostic and Coding Manual. Westchester, USA; American Academy of Sleep Medicine; 2005.
2. Young T, Evans L, Finn L. Estimation of the clinically diagnosed proportion of sleep apnea syndrome in middle-aged men and women. Sleep 1997;20(9):705-6.
Declaration of competing interests: None Declared.


