What do hearing healthcare providers see as the benefits and barriers to delivering speech testing? This article explores the latest research.
Why speech testing?
Speech tests have been used across ENT and audiology practice to measure an individual’s speech recognition thresholds and perception of supra-threshold speech in aided and/or unaided testing conditions, in quiet or in noise. They are commonly used as an outcome measure in auditory research studies, e.g. investigating benefits of hearing devices or effects of auditory training, and prior to hearing aid fitting to capture a listener’s functional ability and identify appropriate intervention strategies.
It is increasingly argued that speech tests provide more ecologically valid (‘real world’) information on the impact of hearing loss on an individual’s communication and quality of life. A recent systematic review, evaluating behavioural assessment methods used before hearing device fitting, reported that patients who underwent speech-in-noise testing were more likely to have higher measures of hearing aid satisfaction [1].
Despite the existence of British Society of Audiology-recommended procedures for key audiological assessment methods, including for pure tone audiometry and speech-in-noise testing, there is a notable absence of one for speech testing in quiet. Prior to our recent publication, there was no data on the use of speech testing in clinical practice by hearing healthcare professionals (HHPs).
SEE ALSO
According to a global survey of audiology practice, audiologists in 46% of countries (n = 62 countries, representing 78% of the world’s population) carried out speech tests (respondents were not asked to report the types of speech tests used) [2]. Inconsistency of speech testing practices between HHPs, audiology centres and countries may impact the interpretability of test results, how trends in patient populations are monitored, and how outcomes are compared between sites, depending on the level of disparity.
Patterns of speech testing in audiological clinical practice
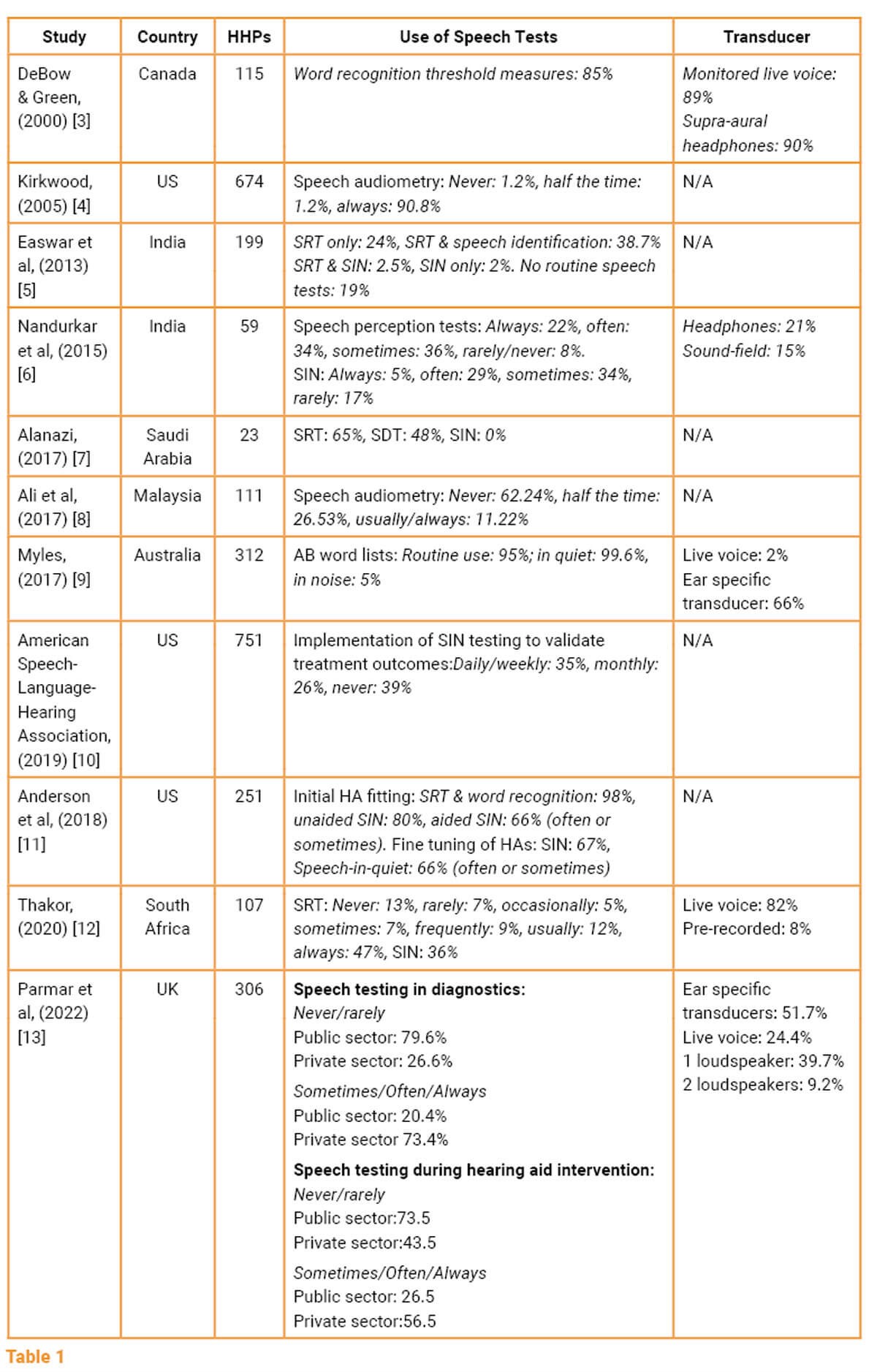
In our recent publication, we (a) collated global speech testing practice patterns from the literature and (b) collected data from UK HHPs through an online survey. A summary of this data is presented in Table 1.
Speech testing: barriers and benefits
Studies summarised in Table 1 identified the following barriers to using speech testing:
- Insufficient clinical time.
- A lack of appropriate speech test materials (e.g. language/accent specific stimuli).
- An absence of normative data.
- No local/national clinical guidance.
Although speech testing is recognised as a functional hearing assessment, the lack of standardisation represents a barrier to its clinical use [14], affecting the consistency of speech testing usage between clinicians and services across the world.
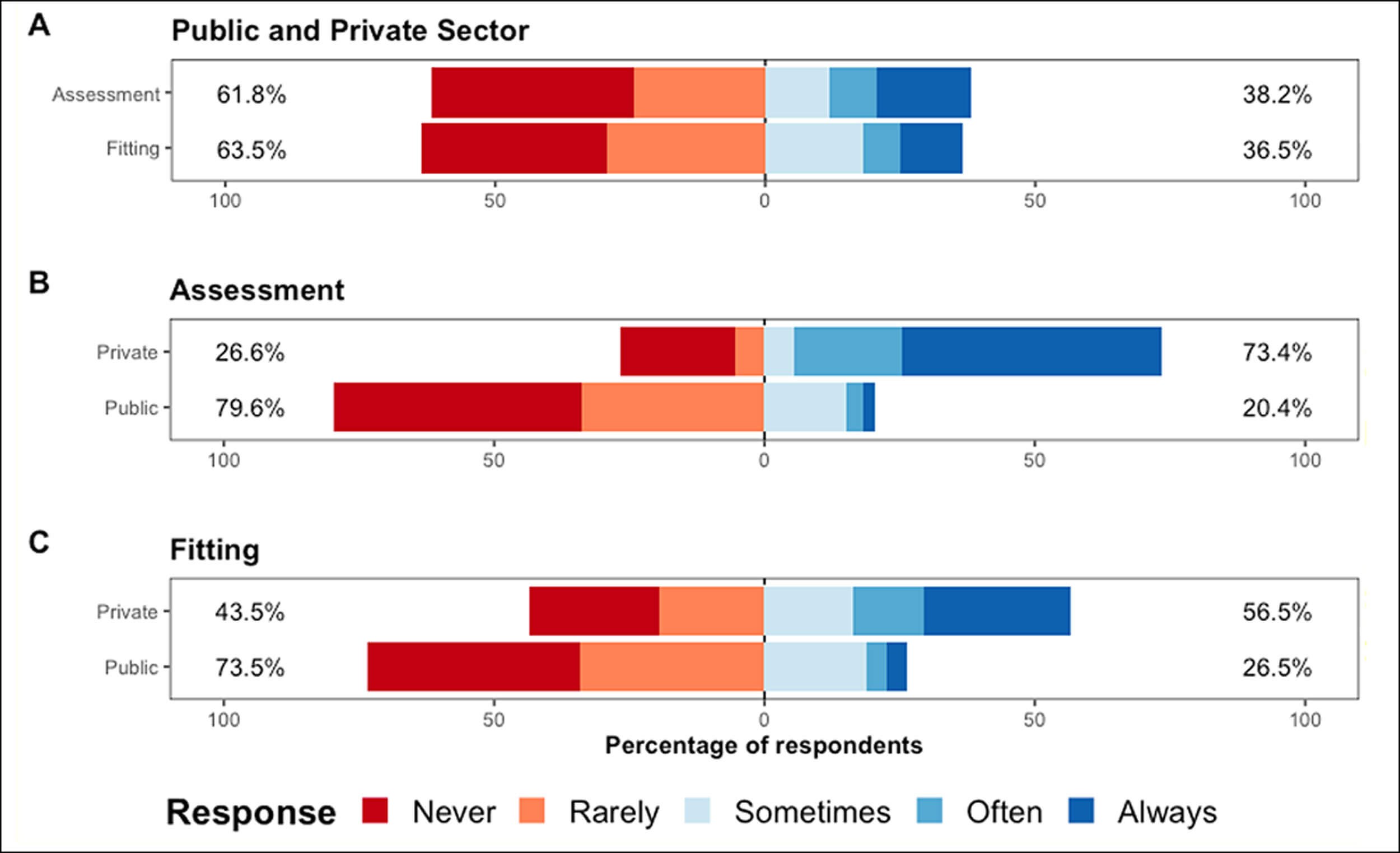
Figure 1. Use of speech testing in the UK (adapted from Parmar et al [13]).
The use of speech testing during hearing aid fittings by UK private and public sector HHPs.
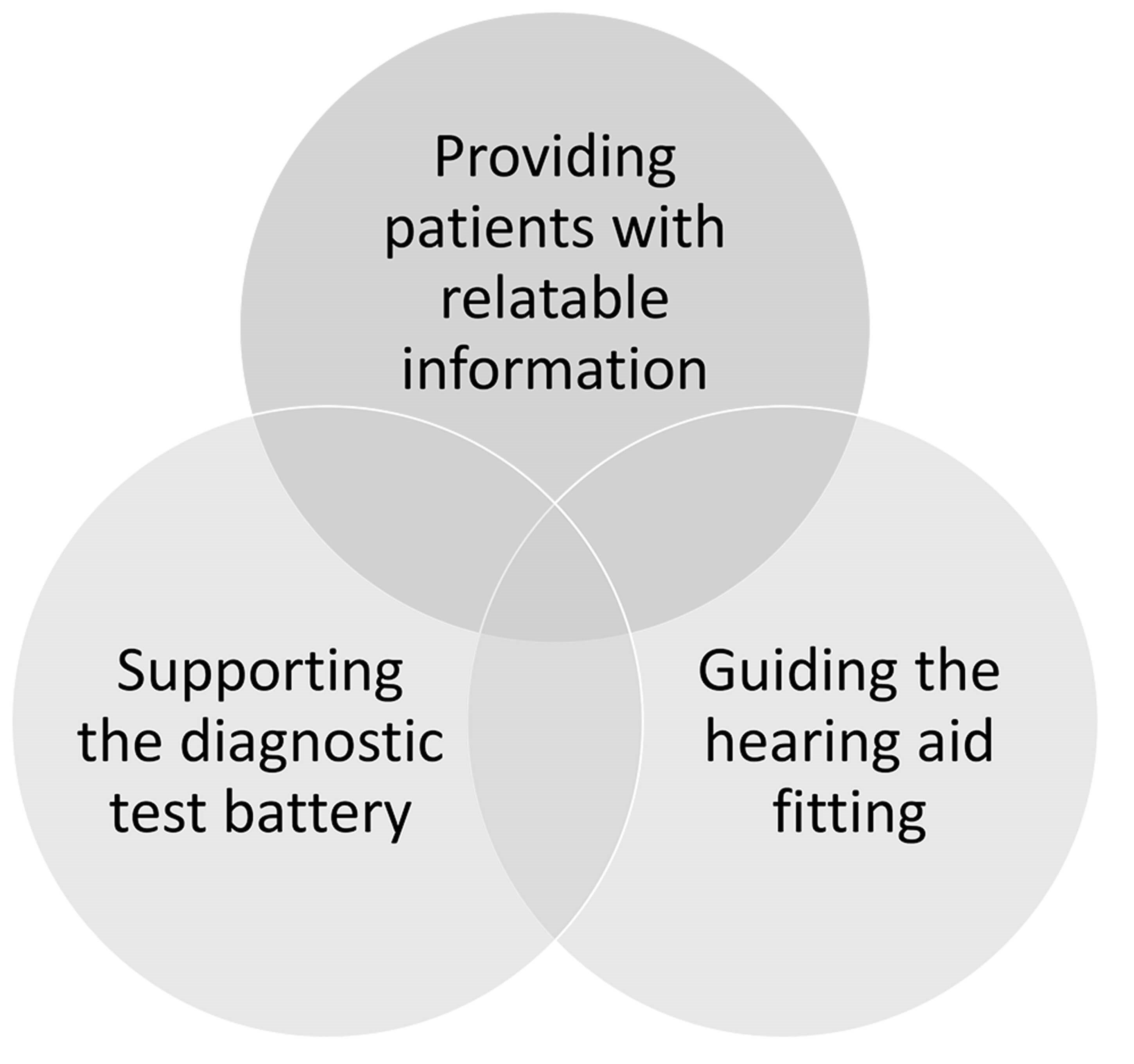
Figure 2. Benefits of speech testing as identified by UK HHPs [13].
UK HHPs reported a range of benefits of speech testing, summarised in Figure 2 [13]. When providing patients with information about their hearing loss, HHPs reported that using speech testing helped convey the message in a more relatable way, compared to explaining the audiogram alone. Speech testing was also reported as being beneficial pre and post hearing aid fitting, and to assist hearing aid fine tuning. Finally, HHPs reported speech testing to be an important part of specific diagnostic test batteries (e.g. auditory processing disorder, non-organic hearing loss, and cochlear implant candidacy).
Conclusion
Use of speech testing by HHPs in the UK reflects the global pattern of variable use. In the UK in particular, public-sector HHPs reported relatively infrequent use of speech testing during the clinical assessment and HA fittings of adult patients (Figure 1). Private sector audiology practices in the UK demonstrated a pattern of uptake more closely resembling the US and Canada.
It is clear that UK HPPs recognise the value of speech testing in audiological assessment and rehabilitation. To address this, there is a need for:
- Time-efficient speech tests.
- Speech stimuli in regional accents/dialects.
- Normative data to support interpretation of results.
- National guidance on the use of speech tests.
Additionally, an international survey to monitor and evaluate use of audiological assessment practices could support the development of standardised approaches.
References
1. Davidson A, Marrone N, Wong B, Musiek F. Predicting hearing aid satisfaction in adults: A systematic review of speech-in-noise tests and other behavioral measures. Ear Hear 2021;42(6):1485-98.
2. Goulios H, Patuzzi RB. Audiology education and practice from an international perspective. Int J Audiol 2008;47(10):647-64.
3. DeBow A, Green WB. A survey of Canadian audiological practices: Pure tone and speech audiometry. Can J Speech-Lang Pathol Audiol 2000;24(4):153-61.
4. Kirkwood DH. When it comes to hearing aids, “more” was the story in ‘04. The Hearing Journal 2005;58(5):28.
5. Easwar V, Boothalingam S, Chundu S. et al. Audiological practice in India: An Internet-based survey of audiologists. Indian J Otolaryngol Head Neck Surg 2013;65(S3):636-44.
6. Nandurkar A, Mukundan G, Gore G. Speech perception assessment practices among audiologists in India: A preliminary survey. Int J Speech-Language Pathol and Audiol 2015;3(2):52‑65.
7. Alanazi AA. Audiology and speech-language pathology practice in Saudi Arabia. Int J Health Sci 2017;11(5):43-55.
8. Ali A, Hickson L, Meyer C. Audiological management of adults with hearing impairment in Malaysia. Int J Audiol 2017;56(6):408-16.
9. Myles AJ. The clinical use of Arthur Boothroyd (AB) word lists in Australia: Exploring evidence-based practice. Int J Audiol 2017;56(11):870-5.
10. American Speech-Language-Hearing Association. Audiology survey report: Private practice 2019
www.asha.org/siteassets/surveys/
2018-audiology-survey-private
-practice-trends.pdf
11. Anderson MC, Arehart KH, Souza PE. Survey of current practice in the fitting and fine-tuning of common signal-processing features in hearing aids for adults. J Am Acad Audiol 2018;29(2):118‑24.
12. Thakor H. South African audiologists’ use of speech-in-noise testing for adults with hearing difficulties [Dissertation, University of the Witwatersrand] 2020.
https://wiredspace.wits.ac.za/
handle/10539/30580
13. Parmar BJ, Rajasingam SL, Bizley JK, Vickers DA. Factors Affecting the Use of Speech Testing in Adult Audiology. Am J Audiol 2022;31(3):528-40.
14. Moore DR, Whiston H, Lough M, et al. FreeHear: A new sound-field speech-in-babble hearing assessment tool. Trends Hear 2019;23:2331216519872378.
Links last accessed March 2023.








