Hearing loss and tinnitus resulting from blast waves in the war zone is becoming more common in our clinics. Hamid Jalilvand based in Tehran, shares his experience in audiological rehabilitation and research findings on patients in his clinics with a focus on the special fitting considerations of hearing aids to improve outcomes in this population of patients.
Blast waves
War zones have many effects on the organs of the human body, and the auditory system is one of these. There are two particularly harmful dangers: the very high level of instant noises and blast wave. Weapons can produce noise levels up to 160 dB (for rifles) or 176 dB [1], which are very dangerous for human beings and even more dangerous in blast wave conditions [2]. Blast waves are the result of changing air pressure due to an explosion [2].
In an explosion, when solid materials are very rapidly converted into gas, positive pressure is followed by negative pressure. The auditory system is most affected by blast waves, especially the peripheral auditory system which is very sensitive to pressure changes [3]. In addition to rupture of tympanic membrane and ossicular chain discontinuity, blast injury causes loss of outer hair cells in base of cochlea and decreases the spiral ganglion neurons [3].





A war veterna with blast induced tinnitus with hearing loss as well as a
severe skin lung problems after exposure to chemical bombs.
Blast-induced tinnitus
There are two main complaints from war noise and blast-induced injury in terms of the hearing system: tinnitus and hearing loss [4]. I mention tinnitus first, because it has such profound effects on patients compared to hearing loss. Subjective tinnitus is the most common complaint among patients with blast injury. Tinnitus is a buzzing or ringing sound heard by the patient without any external source. Our longitudinal study and experience working with patients with war injuries has shown that most of these patients complain mainly about tinnitus. While all of them have a degree of hearing loss, most are less affected by this [5].
Audiological treatment
One of the various treatment and management approaches for tinnitus is audiological treatment, which is very effective. For a patient with blast-induced tinnitus with hearing loss, fitting a hearing aid is usually the most effective and efficient long-term treatment, as shown by our almost 10-year study [5]. It seems that noise- or blast-induced tinnitus is caused by the removal of inhibition in the central auditory system as a result of peripheral auditory deprivation and consequent auditory reorganisation [6]. Thus, if auditory input is restored to the peripheral system (i.e. cochlea and auditory peripheral nerve), inhibition in the central auditory system will be limited.
“Our longitudinal study and experience working with patients with war injuries has shown that most of these patients complain mainly about tinnitus.”
By amplifying sounds and presenting them to the hearing system, a hearing aid can mostly eliminate or at least relieve tinnitus. Our current results show that for a patient with tinnitus and hearing loss, fitting a hearing aid has a greater effect on tinnitus suppression than using a noise generator in the long term [5]. Noise generators, by producing some noise or sound, mask the patient’s tinnitus. Although they are initially very effective at suppressing tinnitus, they are not a good option for long-term treatment of tinnitus via inhibition in the central auditory system [5].
In fact, it seems that fitting a hearing aid has an effect beyond tinnitus suppression. In some cases we have observed that a patient’s tinnitus has not immediately returned after removal of their hearing aid; it can take from 30 minutes to six or seven hours. This phenomenon implies that the amplification of sounds to the injured auditory system does not simply have a suppression effect, but an inhibition effect on tinnitus. More research in this area is needed, however audiologists working in the field of deprivation-tinnitus must take this effect into consideration. The most valuable results from several decades of research in animals show that the cause of tinnitus in central parts of the auditory system is auditory deprivation as a result of peripheral auditory dysfunction [6].
Important clinical considerations
Since hearing aids can suppress or remove the patient’s tinnitus effectively, we have to consider the circumstances which can affect our fitting outcome. Fitting hearing aids for patients with blast-induced tinnitus and hearing loss requires some special considerations, that are not widely found in current literature or fitting rationales. The following are some of the most important aspects which affect our fitting outcomes.
Hypersensitivity to amplification and acclimatisation
A patient with tinnitus probably has severe recruitment and hypersensitivity to relatively loud sounds, which are tolerable for normal hearing people. They are sensitive to amplification of the frequency range, especially when there is a (severe) hearing loss with a steep slope in that range. When a patient has long-term auditory deprivation, it is essential to provide gain gradually over time. In other words, they need to acclimatise to amplification of the affected frequency area. This is different from the normal process of acclimatisation that a typical patient with hearing loss experiences. More time and more gain reduction is needed for acclimatisation to take place in a patient with blast-induced tinnitus [5].
Prescription of frequency response
Because of deprivation-induced hypersensitivity, we have to modify the prescribed frequency response of hearing aids regarding tinnitus frequency. In most patients with blast-induced tinnitus, the frequency of tinnitus is high pitch, and many have high frequency hearing loss. For this reason, some amplification reduction at high frequency is needed at the time of first hearing aid fitting (Figure 1). Although, unfortunately, there is still no approach in hearing aid prescription rationale that considers this effect in patients with severe tinnitus and hypersensitivity, our study has shown that if amplification is reduced for the patient’s comfort, the patient can use the hearing aid and his / her tinnitus is suppressed effectively [5]. The more comfortable a patient is with the amplification, the faster acclimatisation occurs.
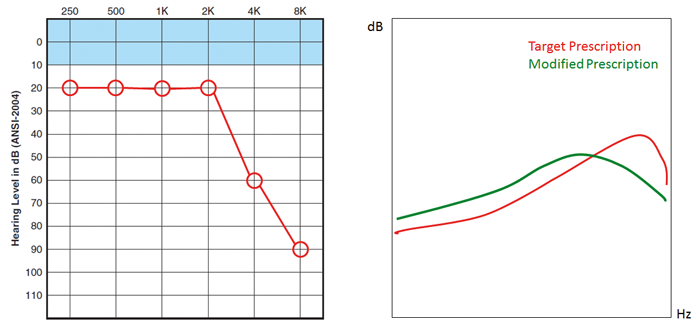
Figure 1. For a patient with blast-induced tinnitus and high frequency hearing loss, it is advisable to modify the gain frequency response prescribed by typical fitting rationale. In this case, the target prescription has more high frequency gain, however the patient’s tinnitus is probably in that range. Because of acclimatisation and tinnitus suppression, gain reduction is needed at high frequency range. Also, increased gain before the audiogram kneepoint (2kHz in this case) could be very helpful in tinnitus suppression.
Amplitude compression and frequency lowering
Regarding hypersensitivity to amplified sounds, severe tinnitus, and amplification of hearing loss region, using a hearing aid with nonlinear amplification of sounds is an ideal strategy in audiological treatment of blast-induced tinnitus. It seems that a fast-acting multi-channel hearing aid with lower compression threshold and relatively higher compression ratio is a good option. Also, frequency lowering, a technique for making the higher frequency sounds audible for patients with a cochlear ‘dead region’ or tinnitus with higher pitch, is a very effective option for tinnitus relief or tinnitus reduction.
Mixed fitting of hearing aid and noise generator
Although a hearing aid is a much stronger instrument for tinnitus relief compared to a noise generator, various hearing instruments are currently available that incorporate both a hearing aid and a noise generator. They are very effective for patients that need to have amplification (because of their hearing loss) and a noise generator (because of their tinnitus or other tinnitus treatment procedures). In current modern hearing aids, at times when there is no input to the hearing aid (e.g. silence at night), amplification is reduced. This causes the patient to ‘hear’ his / her tinnitus. For this reason, a low noise from the hearing instrument can be very effective for tinnitus relief. Although our study has shown that usage of these mixed instruments is increasing amongst patients, amplification of the area of hearing loss and consequent restoration of inhibition in higher auditory centres is the best long-term treatment for a patient with blast-induced tinnitus.
“Blast-induced tinnitus is one of the main complaints of war zone survivors. It is a result of auditory deprivation and removal of inhibition in the central auditory system.”
Final points
A current systematic review of the research into the role of hearing aids and noise generators in tinnitus suppression has indicated that the amplification provided by hearing aids is a very effective treatment in terms of tinnitus relief or suppression [7]. This points to perhaps the most important role of hearing aid amplification in restoration of inhibition in the central auditory system, which has not yet been fully researched. One study has shown that amplification makes patients’ tinnitus louder, however the amplification of sound in areas with hearing loss and tinnitus was nearly 40dB, which is very high for patients with mild hearing loss [8]. As previously mentioned, a patient with tinnitus and hypersensitivity to sound requires a lower gain, especially in areas with hearing loss and severe tinnitus. This suggests more research is needed in this area.
References
1. Altman J. Acoustic weapons. A prospective assessment. Science and Global Security 2001;9:165-234.
2. Wightman JM, Gladish SL. Explosions and blast injuries. Ann Emerg Med 2001;37:664-78.
3. Cho S, Gao SS, Xia A, et al. Mechanisms of Hearing Loss after Blast Injury to the Ear. PLOS One 2013;8:e67618.
4. Cave KM, Cornish EM, Chandler DW. Blast injury of the ear: clinical update from the global war on terror. Mil Med 2007;172:72-30.
5. Jalilvand H, Pourbakht A, Haghani H. Hearing Aid or Tinnitus Masker: Which One Is the Best Treatment for Blast-Induced Tinnitus? The Results of a Long-Term Study on 974 Patients. Audiol Neurotol 2015;20(3):195-201.
6. Eggermont JJ, Roberts LE. The neuroscience of tinnitus. Trends in Neurosci 2004;27(11):676-82.
7. Shekhawat GS, Searchfield GD, Stinear CM. Role of hearing AIDS in tinnitus intervention: a scoping review. J Am Acad Audiol. 2013 Sep;24(8):747-62. doi: 10.3766/jaaa.24.8.11.
8. Vanneste S, van Dongen M, Vree BD, et al. Does enriched acoustic environment in humans abolish chronic tinnitus clinically and electrophysiologically? A double blind placebo controlled study. Hearing Research 2013;296:141-8.
Declaration of Competing Interests: None declared.


