NAL-NL3 modernises hearing aid prescription with modular, evidence-based modules, improving real-world comfort and communication for diverse listening needs.
Hearing aid prescription has long relied on a single, audiogram-based formula to guide amplification. While this approach has delivered reliable outcomes for many patients, it has also revealed consistent limitations in addressing the complexity of real-world listening. The NAL-NL3 Fitting System represents a deliberate shift away from a one-size-fits-most prescription towards a modular, clinically responsive framework that better reflects how patients listen, function and participate in everyday environments.
This article provides practical guidance for ENT surgeons, audiologists and hearing practitioners on applying the NAL-NL3 Fitting System in routine clinical care. Rather than introducing an entirely new philosophy, NAL-NL3 builds on decades of evidence underpinning NAL prescriptions, while offering targeted solutions for long-standing unmet clinical needs [1].
Moving beyond a single-formula approach
The NAL-NL3 Fitting System consists of three components (with more to come):
- NAL-NL3 Prescription, which serves as the primary audiogram-based prescription for everyday hearing aid use
- Comfort in Noise Module
- Minimal Hearing Loss Module
The NAL-NL3 Prescription functions as a hearing aid prescription in the traditional sense, compensating for diagnosed hearing loss based on the individual’s audiometric information. The two modules provide structured, evidence-based adaptations designed to address specific listening challenges that are not adequately captured by thresholds alone. This distinction is important. It clarifies how amplification decisions relate to diagnosis, rehabilitation goals and patient-reported outcomes, while preserving the integrity of prescription-based care (Figure 1).

Figure 1.
The NAL-NL3 Prescription: what has changed?
The core philosophy of NAL-NL3 remains consistent with earlier NAL prescriptions: maximise speech intelligibility in quiet while ensuring overall loudness is no greater than normal hearing. Established fitting procedures, including real-ear verification, maximum output checks and counselling, remain unchanged, allowing seamless integration into current clinical workflows. What differentiates NAL-NL3 [1] from NAL-NL2 [2] is the way the prescription has been refined to better reflect real-world clinical practice. Analysis of large-scale fitting data revealed consistent patterns in how hearing care professionals routinely adjusted NAL-NL2 targets, particularly for certain audiometric configurations. These patterns occurred in cases such as mixed losses and reverse-sloping losses, where prescribed targets were often technically appropriate but clinically difficult to achieve. The adjustments made by hearing practitioners reflected the need to balance intelligibility with comfort and tolerability in everyday use.
NAL-NL3 incorporates this clinical reality into the prescription. Key refinements include:
- More achievable gain targets for mixed and reverse-sloping losses, avoiding excessive low- and high-frequency amplification.
- Refined compression ratios, with a reduced maximum compression ratio and more linear behaviour at mild and profound degrees of loss.
- Rebalanced frequency weighting, reducing emphasis on frequency regions where speech importance is low or targets are rarely met in practice.
For hearing care professionals, this translates to fittings that more closely resemble what would previously have been achieved only after extensive fine-tuning.
During early clinical evaluation, hearing care professionals reported that NAL-NL3 targets were readily achievable in routine fittings, with less need for post-verification fine-tuning and no substantive change to fitting time compared with NAL-NL2. One hearing care professional reflected that there were “lots of very positive responses to the sound of the HAs, with minimal adjustments beyond the NAL-NL3 target settings”. While real-ear verification remains essential, many fittings can now be completed more efficiently, with improved first-fit acceptance.
Comfort in Noise Module: managing listening fatigue
A common clinical presentation is the patient who reports good speech understanding in quiet, yet finds noisy environments overwhelming and fatiguing. These individuals often demonstrate adequate performance on speech-in-quiet measures and their fittings verify well to target, yet continue to experience difficulty hearing in restaurants, meetings or social gatherings.
The NAL-NL3 Comfort in Noise Module was developed specifically for this group. Rather than attempting to increase intelligibility in noise, its primary aim is to improve listening comfort while maintaining access to speech cues. The module applies a loudness-based gain strategy that reduces amplification at moderate and high input levels, particularly in frequency regions where noise contributes most to perceived loudness. Compression behaviour is adjusted to reduce sharpness and listening effort, while preserving audibility for softer speech inputs.
Clinical and laboratory evaluations show that speech intelligibility with the Comfort in Noise Module is comparable to the standard NAL-NL3 Prescription, while perceived comfort and listening pleasantness are significantly improved. In real-world trials, users preferred the Comfort in Noise Module over the Prescription when it provided more naturalness and loudness comfort in noisy situations. One participant commented, “I just found it more comfortable listening”, while another noted, “Overall I preferred [Comfort in Noise program] because of its clarity and comfort”.
As with all NAL-NL3 fittings, verification using real-ear measures remains best practice, with target matching typically performed at conversational and higher input levels (65 and 80 dB SPL for noise-focused modules). If the NAL-NL3 Prescription has been verified, extra real-ear measurements for the Comfort in Noise Module are usually not needed when it is applied within the manufacturer’s fitting software; its gain changes are evidence-based, although hearing care professionals can still choose to verify the Comfort in Noise Module in their REM system if they wish.
Key clinical considerations for the Comfort in Noise Module
Identifying suitable candidates
Patients who benefit from the Comfort in Noise Module typically:
- Report satisfaction with hearing aid performance in quiet;
- Describe discomfort, strain or fatigue in noise;
- Show outcome measures indicating difficulty primarily in noisy environments;
- Show difficulty primarily in noise on outcome measures, such as the Abbreviated Profile of Hearing Aid Benefit (APHAB) on the Background Noise subscale or the Speech, Spatial and Qualities of Hearing Scale (SSQ) on listening effort ratings [3,4].
The Comfort in Noise Module should only be introduced after the NAL-NL3 Prescription has been fitted and fully verified as the everyday program. Counselling is essential. It is best positioned as a secondary, situational option rather than a replacement for the primary fitting. Patients should understand that the module is designed to improve comfort rather than eliminate background noise or guarantee improved speech intelligibility in all situations.
Minimal Hearing Loss Module: extending care beyond the audiogram
An increasing number of adults present with communication difficulties, despite having normal or near normal audiometric thresholds. These individuals commonly report difficulty understanding speech in noise or group settings. However, traditional prescriptions typically provide little or no gain, leaving hearing care professionals with limited technological options beyond counselling and communication strategies.
The NAL-NL3 Minimal Hearing Loss Module addresses this gap by offering conservative, evidence-based gain targets that allow individuals with minimal hearing loss to benefit from directional microphones, beamforming and noise-reduction features [1]. When all thresholds are in the normal range, the module prescribes modest gain, typically in the range of 3–4 dB from 1–4 kHz, with linear amplification at conversational levels and carefully managed maximum output to ensure safe exposure during situational use.
The intent is not to treat hearing loss, but to support communication in demanding listening environments. During take-home trials, participants shared how they used the hearing aids in specific situations. One noted wearing them “whenever I went out — choir rehearsal, movies, dinner etc”. Another shared that they “wore them to shopping centres two or three times a week and to cricket on weekends”. A third participant explained, “I used the hearing aids daily, mainly in my workplace”.
Key clinical considerations for Minimal Hearing Loss fittings
Identifying suitable candidates
Fitting patients with minimal hearing loss requires different clinical emphasis from conventional amplification:
- Candidacy is driven by self-reported difficulty, not audiometric thresholds alone.
- Coupling choice is critical. More occluding fittings often provide greater benefit by ensuring the processed signal dominates over the direct acoustic path.
Expectations must be carefully managed. The device is intended for situational use in specific noisy environments, not continuous all-day use. In noise, more occluding couplings can often be tolerated, with own-voice effects generally less noticeable than in quiet, all-day listening. Verification remains best practice. Measuring gain at conversational and higher input levels confirms that prescribed targets are met and that the coupling provides the intended acoustic effect. Attention should be given to mid- and high-level inputs where clinical benefit is most likely to occur.
A practical decision framework
The modular structure of NAL-NL3 supports a clear, needs-based clinical workflow:
- Measured hearing loss present
→ Fit and verify the NAL-NL3 Prescription as the everyday program. - Persistent discomfort or fatigue in noise despite a verified fitting
→ Add the Comfort in Noise Module to the NAL-NL3 Prescription as a situational option. - Normal or near-normal thresholds with functional difficulty
→ Consider selecting the Minimal Hearing Loss Module, instead of the NAL-NL3 Prescription, for targeted, situational use.
This approach allows hearing care professionals to explain recommendations clearly to patients and to justify fitting decisions based on functional outcomes rather than audiograms alone (Table 1) .
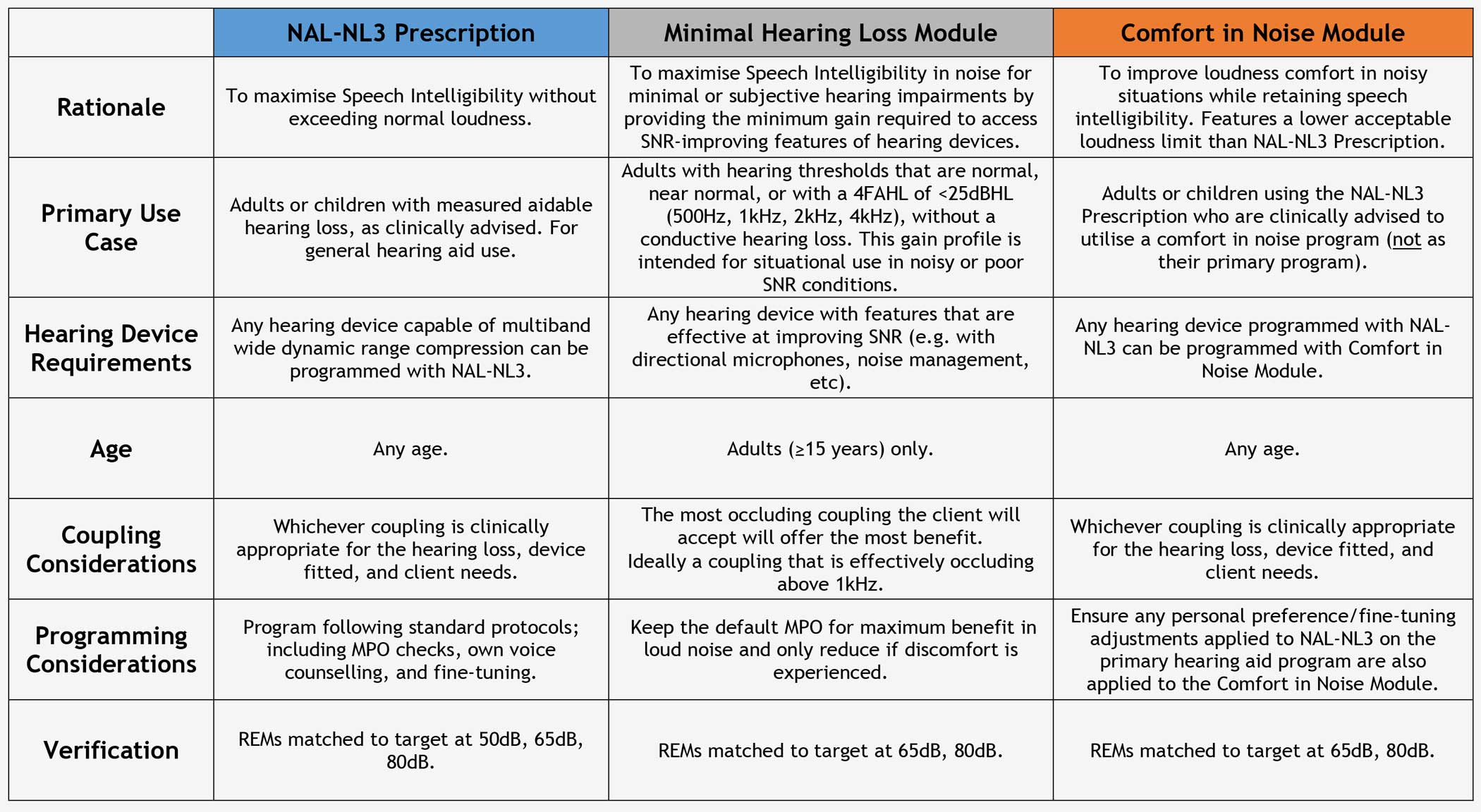
Table 1: NAL-NL3 Cheat sheet for hearing care professionals [5].
Implications for ENT and audiology practice
NAL-NL3 provides a clearer framework for understanding and supporting patients with similar audiograms that may experience very different real-world difficulties and how those difficulties can be addressed through structured amplification strategies. For audiologists, it offers tools that align more closely with contemporary person-centred care, without disrupting established verification and fitting workflows (Table 2).
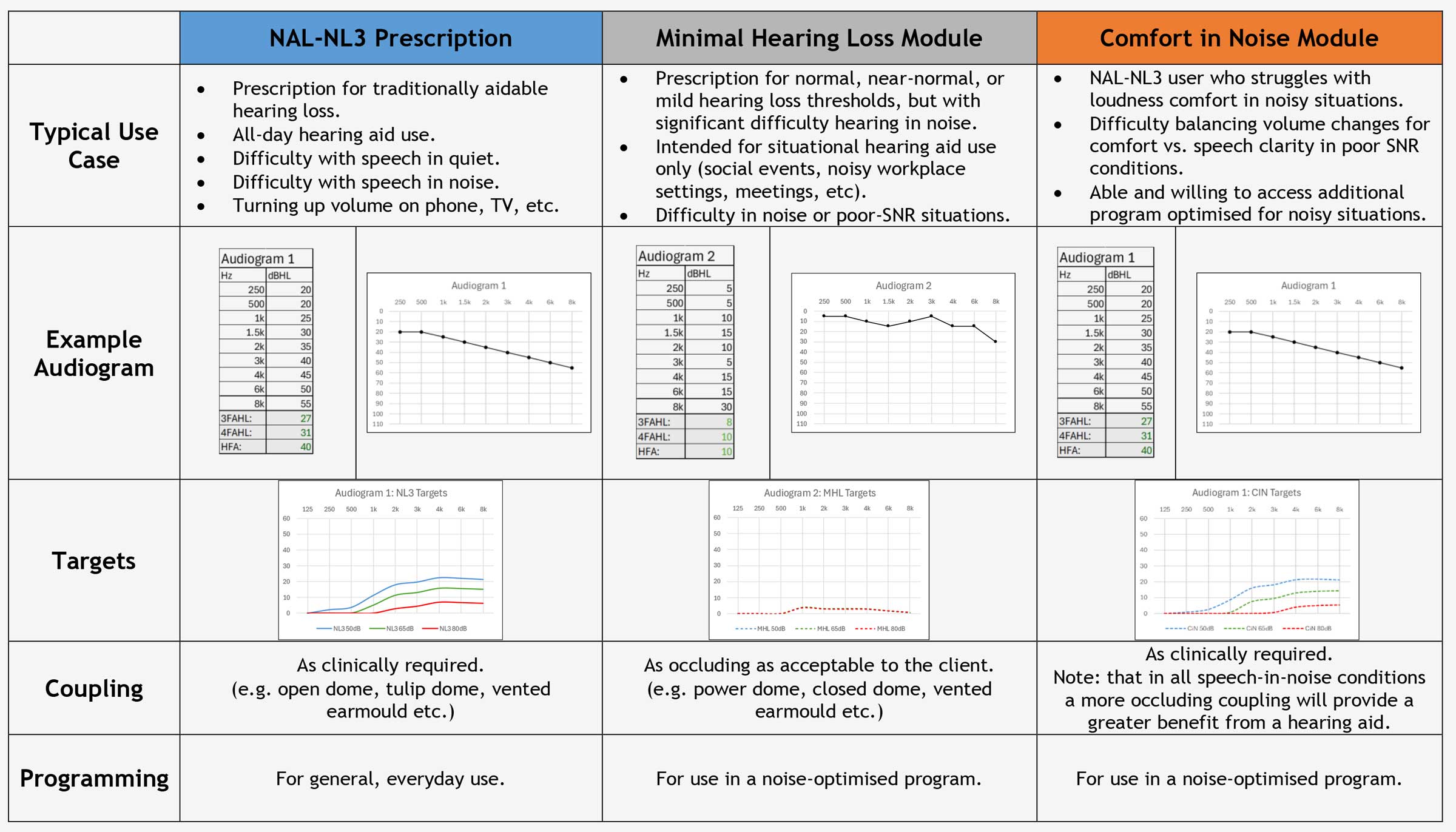
Table 2: Case examples.
For more detailed information, please visit https://nal-nl3.com.au/resources/ which has the NAL-NL3 FAQs for Clinicans and NAL-NL3 Cheat Sheet for hearing care professionals available for download, plus other information and publications.
"The NAL-NL3 Fitting System represents a deliberate shift away from a one-size-fits-most prescription towards a modular, clinically responsive framework that better reflects how patients listen, function and participate in everyday environments"
Conclusion
NAL-NL3 represents an evolution in hearing aid prescription, not by abandoning established principles, but by extending them into a modular system that reflects real-world listening demands. By combining the refined core prescription and introducing targeted modules for comfort in noise and minimal hearing loss, NAL-NL3 enables hearing care professionals to deliver more personalised, clinically relevant care. In doing so, NAL-NL3 bridges the gap between audiometric diagnosis and lived communication experience, supporting more clinically relevant hearing care.
References
1. Croteau M, Kwok C. Using NAL-NL3 in clinical practice: a modular NAL fitting system for real-world listening needs. Int J Audiol. Under review.
2. Keidser G, Dillon H, Flax M, et al. The NAL-NL2 Prescription Procedure. Audiol Res 2011;1(1):e24.
3. Cox RM, Alexander GC. The abbreviated profile of hearing aid benefit. Ear and Hearing 1995;16(2):176–86.
4. Gatehouse S, Noble W. The speech, spatial and qualities of hearing scale (SSQ). Int J Audiol 2004;43(2):85–99.
5. NAL-NL3 Clinicians FAQ and NAL-NL3 Cheat sheet for Clinicians (2025).
https://nal-nl3.com.au/resources/
[Link last accessed April 2026].
Declaration of competing interests: None declared.








