Are they a malingerer? Or perhaps they are inattentive? It may be their drugs! Robert DiSogra considers the side-effects of medication on the test subject.
The audiogram serves many purposes in clinical practice. For the audiologist, it helps to differentiate between conductive, sensorineural or mixed type hearing losses. It also serves as a counselling tool for persons when communication complaints are not supported by the audiometric data (i.e. an auditory processing deficit). For the otolaryngologist, it is the stepping stone for additional diagnostic tests, pharmacological intervention and / or surgery [1].
In addition to the audiogram, differentiating between peripheral or central vestibular disorders is critical in developing a management strategy for the patient.
There are over 2000 drugs and more than 400 side-effects that could impact the accuracy of the audiometric or vestibular evaluation as well as impacting the recommendations made for intervention and management [2,3].
Case history
Estimates range from five to eight as to the number of drugs the average elderly person takes daily. Some of these medication side-effects might have the patient not fully understand the test instructions or stay focused on the required task for a particular test. For example, some medications for cardiac patients might have an auditory side- effect (i.e. tinnitus) or might affect vestibular testing (oculomotor dysfunction).
Table 1 is a partial list of reported side-effects that could affect audiometric / vestibular testing.
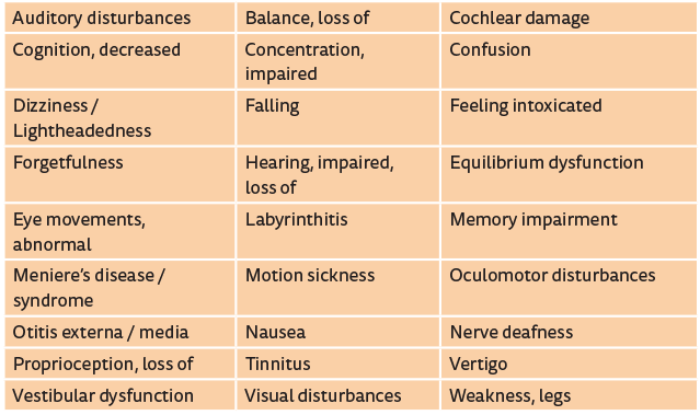
Table 1. Partial list of reported side effects that could affect audiometric / vestibular testing. Incidence figures appear in the PDR for Prescription Drugs or can be obtained from the drug’s manufacturer.
Patient accuracy
Approximately half of the side-effects listed in Table 1 can influence a vestibular study. Therefore, is your patient really a poor test taker? Or not cooperating? Are you suspecting malingering? What recommendations will be inappropriate if side-effects are not looked at?
Timelines
Whether you are conducting a routine audiometric evaluation, a vestibular study or a tinnitus evaluation, establishing a timeline from when the symptoms first began and when the drug was started should be the focus of your case history and differential diagnosis.
“We rely on word recognition scores for many reasons, especially hearing aid candidacy. Therefore, we must recognise that there are many drugs that have cognitive side-effects which may influence the test scores.”
If you believe that the patient is a good historian, remember, ‘memory impairment’ is a drug side-effect. A phone call to the referring physician or the patient’s pharmacist will help you get the start date of the particular drug in question.
Audiogram accuracy – pure tones and speech
So how do we really know that a pure tone threshold is truly a ‘threshold’ for an older patient? We don’t. For example, your 80 year old patient presents with a flat 70dB sensorineural loss with some high frequency roll-off. But during the case history she is not raising her voice or leaning in to hear better. She is answering your questions appropriately even when your mouth is not visible to her. Is that 70dB loss real? Or is it a 35-40dB loss influenced by poor listening skills or an inability to stay focused on the task because of an adverse drug reaction?
Another dilemma is when masking is introduced into the test protocol. Two competing stimuli might be an acoustic overload for an older patient. Are those air-bone gaps real?
We also rely on word recognition scores for many reasons, especially hearing aid candidacy. Therefore, we must recognise that there are many drugs that have cognitive side-effects (see Table 1). The possibility exists that these medications might be influencing the test scores. Fatigue influences concentration. You may need to use a shorter word list. Subsequently, data can be misinterpreted as a ‘change’ – but it might not be a true change.
Geriatric cognitive correction
Although not supported by any scientific studies, clinically, you may want to consider deducting 5-10dB from the ‘reported threshold’ for any octogenarian (or older) to compensate for the possibility, if not probability, that the audiogram is not accurate because of cognitive decline (i.e. poor listening). Over-fitting with hearing aids could occur if you take the audiogram at face value.
Vestibular and tinnitus management
Again, you must establish timelines from when the tinnitus started and when the medication was started. But don’t rely 100% on your patient remembering the start date - a side-effect might also be confusion or memory impairment. Call their pharmacist.
Wrong diagnosis = wrong intervention
Your confidence level must be very high when making recommendations for medical or surgical intervention or hearing aid intervention. Is the loss truly sensorineural? Do other tests support conductive hearing loss or mixed hearing loss? Are the abnormal eye movements truly vestibular-related or central?
“Incidence figures for some side-effects can be very small but nonetheless they must be considered when there are test discrepancies.”
Look back at those patients who could not adjust to amplification. How well did we counsel them? First time user expectations? Too much background noise? Was it them or did you miss something? Did you interpret the audiogram at face value? That ‘something’ might be the accuracy of their test which might have been influenced by an adverse drug reaction in addition to their cognitive abilities.
Reporting your findings and suspicions
Document everything. Report the data as you see fit but also report your concerns about accuracy, discovery of drug timelines and any observations of behaviour during the testing that might have influenced your findings (and your recommendations).
Summary
No one is knowledgeable of all the FDA approved drugs and their side-effects. However there are reliable websites available that provide accurate and up-to-date information about side- effects. Contacting a drug’s manufacturer is simple and you might find some additional information that could be helpful to you and your patient [4,5]. If in doubt, call the patient’s pharmacist. Incidence figures for some side-effects can be very small but nonetheless they must be considered when there are test discrepancies.
Suggestions to reduce the possibility of drug influences on audiological testing
- Spend more time in getting an accurate case history. If the patient cannot recall the name(s) of the drug(s) they are taking, call their pharmacist
- Reference www.rxlist.com, www.drugs.com, www.earserv.com/drugs or www.epocrates.com
NOTE: these websites are not an endorsement by the author or publisher - Establish timelines from when the problem began and when the drug(s) were prescribed. This is imperative for tinnitus patients and patients reporting vestibular problems
- Make certain that your patient understands the test instructions (with a demonstration if necessary)
- Never forget what you learned in Audiology 101 about test / retest reliability
- A partial word recognition list may be necessary
References
1. Zubick HH, DiSogra RM. Basic assessment of auditory function. In: Branch WT, (Ed.). Office Practice of Medicine, 2nd edition. Philadelphia, USA; Saunders; 1987.
2. DiSogra RM. Adverse drug reactions and audiology practice, Audiology Today Special Issue, American Academy of Audiology, September, 2001.
3. DiSogra, RM. Adverse drug reactions and audiology practice, Audiology Today, American Academy of Audiology, September, 2008.
4. DiSogra, RM. Staying current: website and resources for pharmacological information. In Campbell KCM, (Ed.). Pharmacology and Ototoxicity for the Audiologist. Demler Learning; 2006.
5. DiSogra RM. Adverse Drug Reactions: Issues and Answers for the Audiologist CE series, Audiology Online.
http://www.audiologyonline.com/articles/
adverse-drug-reactions-issues-and-1094
Last accessed September 2016.
Declaration of Competing Interests: None declared.


