Hearing loss has a well-documented adverse impact on emotional, social and physical well-being. In this article, Dr Piers Dawes from the University of Manchester gives an insight into his team’s recent work analysing the very large UK Biobank data set, with specific reference to adults between 40 and 69 years of age.
Hearing loss has a substantial adverse impact on emotional, social and physical well-being. Hearing loss is usually measured in terms of audiometric measures, which estimate the quietest intensity at which tone beeps of various pitches can be detected. However, associations between such audiometric measures and measures of hearing disability are surprisingly modest.
Some have advocated the use of tests of speech recognition as a supplement to audiometric measures; difficulty with speech in noise is the primary complaint by people with hearing loss, so tests of speech recognition in noise could provide an ecologically valid measure of hearing.
Surprisingly, descriptions of hearing in population-based samples using tests of speech recognition in noise are exceedingly rare. We recently described speech recognition in noise performance in the very large UK Biobank data set [1], which included speech recognition data (based on the digit triplet test [2]) for 164,770 UK adults aged between 40 and 69 years [3]. Impaired hearing was identified if speech recognition in noise performance was well outside the normal range (poorer than two standard deviations), compared to a normative sample. This level of performance would correspond to significant hearing difficulties in both home and work life.
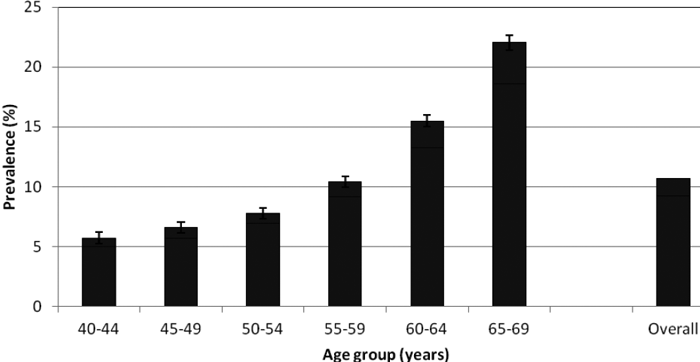
Figure. 1. Prevalence (%) of hearing disability based on Digit Triplet Test performance in the better ear by age group.
Error bars show the 95% confidence interval for performance outside the normal range.
(Figure reproduced from Dawes et al 2014.)
Hearing impairment, tinnitus and hearing aid use
Overall, 10.7% of adults had impaired hearing (Figure 1). The proportion of adults with impaired hearing begins to rise steeply after around age 50 years. The proportion of people who reported tinnitus was 16.9% overall. The proportion of people with tinnitus also increased with age, although there was a more gradual increase with age than for poor hearing.
“Hearing loss is a condition with very high prevalence and significant burden, entrenched socioeconomic and ethnic inequality, and persistent low uptake and use of hearing aids.”
Only 2% of adults reported using a hearing aid. The last time hearing aid use in the general UK population was measured was in the early 1980s; hearing aid ownership was 2.8% among 41-70-year-olds (compared to an estimated 9.4% of the population in that age range who had hearing loss severe enough to benefit from a hearing aid [4]). Despite advances in hearing aid technology and improvements in service provision, it seems that hearing aid uptake and use has not improved substantially in the last 30 years. Recent reviews surveyed reasons for low hearing aid uptake and use, which include motivation, expectation, attitude to hearing aids, hearing sensitivity and the effect of counselling, uncomfortable fit and lack of perceived benefit [5, 6]. Low uptake/use may be addressed by i) making hearing care a ‘lifestyle choice’ by removing the need to obtain a referral from a GP to go to a hospital-based audiology clinic (which may contribute to the stigmatisation of hearing loss by association with infirmity) and making quality audiology services more accessible; ii) undertaking good-quality trials of adult hearing screening and intervention based on models of hearing aid uptake and use, and iii) improving hearing aid technology to a point where it will significantly improve speech understanding in noise, so doing away with a major reason for non-use.
Demographics of hearing
We examined demographic factors, such as ethnicity, sex and socioeconomic status as well as noise exposure. Both work-related and music-related noise exposure were associated with greater likelihood of poor hearing. The data suggested that music-related noise exposure may pose a risk to hearing similar to risks established for occupational noise exposure.
Previous research in the US found that African Americans tended to have better hearing than White Americans. The suggested reason was that melanin may have a protective effect against hearing loss in the cochlea. We therefore expected that people with a non-White ethnic background would have better hearing than people with a White British background. In our analysis, a surprising result was that non-White ethnicity was associated with poorer hearing. The association between non-White ethnicity and poor hearing remained when we were only including people who had been born in the UK, so the association is probably not due to poor English language ability. The ethnic sub-groups who were most at risk of poor hearing were the ones that had been previously identified as having poor general health (Bangladeshi, Black African, Black Other and Pakistani [7]).
Rates of hearing aid use were also lower among non-White ethnic groups than in the White British population. Suggested reasons for the poor general health of ethnic minorities in the UK centre on culture, lifestyle, socioeconomic factors, reduced uptake of services and biological susceptibility. A similar range of factors may underlie hearing health inequality. Understanding these factors would be a first step towards addressing hearing health inequality. Previous population-based studies of hearing have tended to find that men have poorer hearing than women. However, in our analysis, males were at no higher risk of poor hearing than women. That male sex is not a consistent risk for poor hearing across studies might suggest that there are differences in unmodelled confounding factors associated with sex that vary across populations, and that the risks for poor hearing in men may be modifiable. Interestingly, in the US Health Aging and Body Composition Study [8], sex differences disappeared after adjusting for lifestyle factors such as smoking and work-related noise exposure. It might also be that there is less difference in hearing between men and women in younger age cohorts.
Previous population-based studies of hearing surveyed a generation that included men who had seen military service in WW2 (and been exposed to gunfire noise) and had been employed in ‘traditional’ occupations in farming and manufacturing (and received high levels of occupation-related noise exposure). Younger generations of males may not have such significant cohort-specific experiences. Sex differences in hearing may not be as large as we previously thought. Socioeconomic status was associated with poor hearing, and this has been observed in several studies previously. Low socioeconomic status is associated with occupations involving higher levels of noise exposure. Low socioeconomic status is also associated with a range of factors such as smoking, excessive drinking, poor diet and lack of exercise. All of these factors are linked with hearing loss. Encouragingly, all of these factors are modifiable, so there is scope to reduce levels of hearing loss by addressing these modifiable risks.
Interestingly, it seems that it may not only be socioeconomic status-related risks in adulthood that impact on hearing. A previous study found that socioeconomic status in childhood was associated with a larger variance in adult hearing than socioeconomic status in adulthood, even after accounting for noise exposure, smoking and drinking [9]. Early childhood and prenatal experiences are associated with a range of adult health outcomes [10]. Understanding and reducing the adverse impact of socioeconomic status on adult hearing may require attention to the experiences of childhood.
Challenges of hearing loss
Hearing loss is common and has a substantial adverse effect on quality of life. As health professionals and as a society, we face a daunting challenge. Hearing loss is a condition with very high prevalence and significant burden, entrenched socioeconomic and ethnic inequality, and persistent low uptake and use of hearing aids, the primary treatment for hearing loss. Understanding these challenges is a first step to successfully overcoming them.
References
1. Collins R. What makes UK Biobank special? The Lancet 2012;379(9822):1173-4.
2. Smits C, Kapteyn TS, Houtgast T. Development and validation of an automatic speech-in-noise screening test by telephone. Int J Audiol 2004;43:15-28.
3. Dawes P et al. Hearing in middle age: a population snapshot of 40-69 year olds in the UK. Ear and Hearing 2014;35(3).
4. Davis AC. Hearing in Adults 1995; London: Whurr Publishers Ltd.
5. McCormack A and Fortnum H. Why do people fitted with hearing aids not wear them? Int J Audiol 2013;52(5):360-8.
6. Vestergaard Knudsen L et al. Factors influences help seeking, hearing aid uptake, hearing aid use and satisfaction with hearing aids: a review of the literature. Trends in Amplif 2010;14(3):127-54.
7. Department of Health. Health Survey for England 1999: The health of minority ethnic groups. 2001; http://webarchive.nationalarchives.gov.uk/
+/www.dh.gov.uk/en/
Publicationsandstatistics/Publications/
PublicationsStatistics/DH_4009393.
8. Helzner EP et al. Race and sex differences in age-related hearing loss: the health, aging and body composition study. J Am Geriat Soc 2005;53(12):2119-27.
9. Davis AC, Ecob R and Smith P. The relationships between work-based noise over the adult life course and hearing in middle age. Int J Audiol 2008;47:100-8.
10. Barker DJP. The developmental origins of well-being. Philosophical Transactions of the Royal Society 2004;1359-66.
Declaration of Competing Interests: None declared


