Somatosensory tinnitus occurs when a head, neck or jaw problem influences what the tinnitus sounds like. Audiologists and physical therapists work together to address this tinnitus subtype.
Background
Tinnitus is the perception of sound in the ears or head, in the absence of an external stimulus. Global estimates of tinnitus prevalence reveal that over 740 million adults have tinnitus [1]. There are multiple types of tinnitus, with the most common type known as primary (i.e. subjective) tinnitus, defined as idiopathic, that may or may not be associated with sensorineural hearing loss [2].
The focus of this article is on a subtype called somatosensory tinnitus (ST), which is suspected when the perceptual characteristics (e.g. loudness, pitch) reliably change with head, neck, and/or jaw manoeuvres linked to an underlying biomechanical deficit such as cervical spine injury or temporomandibular joint (TMJ) dysfunction [3].
Current best practices for treatment-seeking patients with tinnitus do not routinely involve an in-depth tinnitus assessment. When reviewing the case history with patients, if tinnitus onset is associated with head or neck injuries, an audiologist might ask follow-up questions about possible fluctuations in the loudness or pitch with head/neck/jaw movements. However, there is no clinical consensus on standard screening procedures or questions to identify ST that would prompt referral to a physical therapist, ideally one who specialises in orthopaedics. The goal of this article is to increase awareness of ST as well as the benefit of taking an interdisciplinary approach involving audiology and physical therapy (physiotherapy; PT) care providers in the assessment and treatment of patients with ST.
ST indicates there is a co-occurring musculoskeletal issue influencing the tinnitus perception. This is why it is recommended an audiologist and physical therapist work together to help patients with ST. Although there are many effective therapeutic approaches to help people live better with tinnitus, there is no evidence of an effective treatment or approach to cure it. ST is unique in that resolving the underlying musculoskeletal issue may also alleviate the tinnitus to some degree, something very much worth exploring.
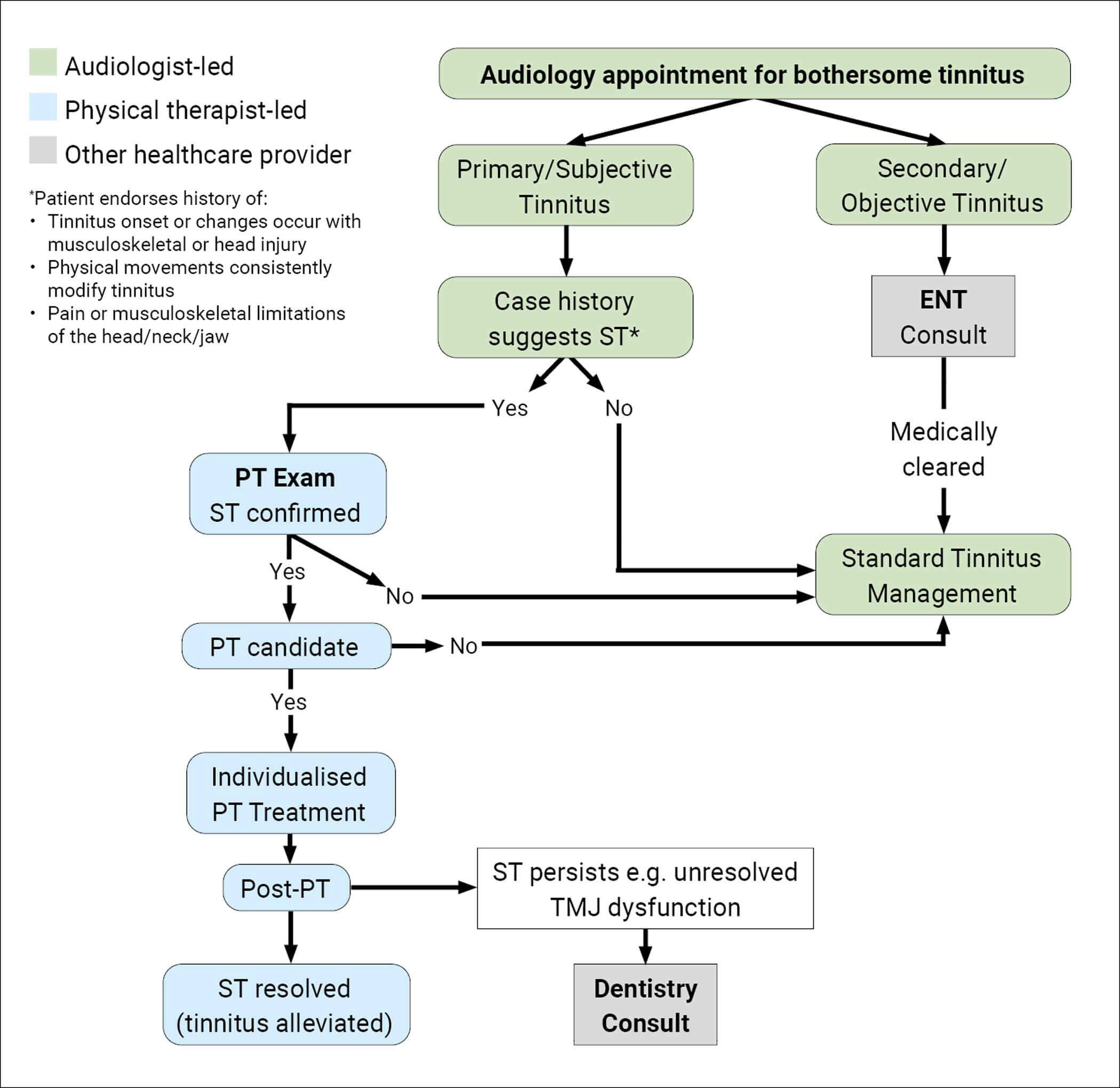
Figure 1: Care Pathway.
Care pathway
Figure 1 shows an interdisciplinary care pathway with the patient first being seen in audiology. When taking a case history for patients with tinnitus, it is important to note if they also have head or neck injuries/pain, TMJ dysfunction or head trauma; if so, it increases the likelihood that their tinnitus could be ST [4]. In these instances, it is recommended that the clinician consider asking follow-up questions and/or having the patient do a few manoeuvres – with the clinician visually verifying what they are doing – to determine if somatic manoeuvres influence the patient’s tinnitus characteristics. If the tinnitus gets louder or softer and/or changes in pitch or location, have the patient repeat the manoeuvre to see if the tinnitus changes are reproducible.
Because one of the aspects of ST is a musculoskeletal impairment linked to the tinnitus, if the audiologist suspects ST, the next step is to refer the patient for a full PT evaluation. The physical therapist will then determine if all the criteria for ST are present or not. The first criterion is to identify if there is a co-occurring biomechanical deficit influencing the patient’s tinnitus. Examples include cervical spine joint mobility restrictions or pain; cervical, upper thoracic or jaw muscle weaknesses; TMJ dysfunction, etc. It is recommended that the standard PT biomechanical exam be modified to include asking about simultaneous changes in the patient’s tinnitus during each part of the evaluation: 1) active and passive cervical, thoracic and TMJ range of motion and joint mobility; 2) strength testing of cervical and jaw musculature and muscular palpation; 3) endurance of deep neck flexor muscles; 4) neurodynamic functional mobility of cervical spine; and 5) body position changes (e.g. sitting to laying down). The caveat here is not all physical therapists are aware of the phenomenon of ST, which is why it is imperative to increase awareness of this tinnitus subtype.
During the PT exam, the physical therapist will determine if a musculoskeletal impairment is present and, if so, if it is associated with the patient’s tinnitus. To determine if a somatic manoeuvre changes the patient’s tinnitus, it is important to have the patient evaluate if their tinnitus changes during the manoeuvre, rather than have them tell you after the exam if their tinnitus changed. The physical therapist should ask the patient to simultaneously evaluate for perceived changes in tinnitus loudness, pitch and/or location (i.e. where the tinnitus is perceived).
It is not uncommon for people to confuse constructs of pitch and loudness, so it is important the wording of your instructions are clear and understood. Regardless of your specialty, as you observe the patient performing manoeuvres, make sure how they respond is consistent with your instructions. For example, when asking if the tinnitus changes in any way, emphasise you want them to focus on changes in what it sounds like during the assessment, and not what it sounded like earlier in the day or other types of fluctuations they might experience. From the audiologist’s perspective, anything that influences the patient’s tinnitus is important to document in the case history. From the physical therapist’s perspective, it is important that the PT exam captures changes in the patient’s tinnitus characteristics that occur during each step of the physical exam to determine if those changes coincide with a musculoskeletal deficit. Once ST is confirmed, the next thing is for the physical therapist to determine if the patient is a candidate for PT.
Additionally, increasing awareness of ST is important because of instances where a patient is seen in PT before audiology. For example, consider a patient being seen in PT for complaints of dizziness. In this common scenario, reporting tinnitus does not typically result in additional testing unless the physical therapist suspects it to be a symptom of another condition (e.g. Ménière’s disease) and refers the patient to otolaryngology. Figure 1 includes case history questions that, if endorsed, warrant follow-up to determine if ST is present.
Conclusions
There are three main criteria that, considered separately, suggest ST but to confirm ST, all must be present: 1) the patient’s tinnitus is modulated by head, neck and/or jaw manoeuvres; 2) the patient’s tinnitus is associated with head/neck/jaw trauma or pain; and 3) presence of biomechanical deficit(s) in the head/neck/jaw regions.
As specified in the interdisciplinary care pathway for ST (Figure 1), if the physical therapist confirms ST and the patient is a candidate for PT, the next step is to create an individualised treatment plan to address the underlying biomechanical deficit and see if improvement with that issue resolves the ST to any degree. At the end of PT, if the biomechanical issue has resolved but the ST is still present, consider if multiple issues were initially present but only one has now resolved. For example, if cervical range of motion improved, but TMJ dysfunction continued, this would necessitate the patient seeing dentistry as a next step. If the ST resolved, but the tinnitus persists and is still bothersome, the patient should be referred back to audiology for additional tinnitus care services.
ST symptom severity, like other types of tinnitus is most likely influenced by multiple intrinsic and extrinsic factors. Additional research is needed to identify other sensory and perceptual contributing factors. Overall, auditory symptoms following head injury, like ST, are poorly understood [5]. Additionally, tinnitus symptoms can be exacerbated by co-occurring health conditions (e.g. post-traumatic stress disorder, hyperacusis, noise sensitivity, etc.) and other health conditions. Therefore, future work is needed to identify prognostic factors, considering auditory and non-auditory factors that, if present, increase the likelihood of a successful treatment outcome.
References
1. Jarach CM, Lugo A, Scala M, et al. Global Prevalence and Incidence of Tinnitus: A Systematic Review and Meta-analysis. JAMA Neurol 2022;79(9):888–900.
2. Tunkel DE, Bauer CA, Sun GH, et al. Clinical practice guideline: Tinnitus. Otolaryngol Head Neck Surg 2014;151(Suppl.2):S1–40.
3. Sanchez TG, Rocha CB. Diagnosis and management of somatosensory tinnitus: review article. Clinics (Sao Paulo) 2011;66(6):1089–94.
4. Michiels S. Somatosensory tinnitus: recent developments in diagnosis and treatment. J Assoc Res Otolaryngol 2023;24:465–72.
5. Theodoroff SM, Papesh M, Duffield TC, et al. Concussion Management Guidelines Neglect Auditory Symptoms. Clin J Sport Med 2022;32(2):82–5.
Acknowledgements
This material is the result of work supported by a Department of Veterans Affairs (VA) Rehabilitation Research Development & Translation Merit Award (#I01RX003924; Theodoroff), a Department of VA OAA Polytrauma/Epilepsy Fellowship (Brodsky) and with resources and the use of facilities at the VA National Center for Rehabilitative Auditory Research (Center Award #I50RX002361) at the VA Portland Health Care System in Portland, Oregon. The contents herein are the opinions of the authors and do not represent the views of the US Department of Veterans Affairs, Department of Defense or the United States Government. This work was prepared as part of official duties as US Government employees and, therefore, is defined as U.S. Government work under Title 17 U.S.C.§101. Per Title 17 U.S.C.§105, copyright protection is not available for any work of the US Government.
Declaration of competing interests: None declared.









