Sudeb Mandal, a GP with special interest in ENT, talks about the novel approach taken in the community to deliver ENT services in Kent in the UK.
The Kent Community ENT service was born with the vision to bring together a community of local ENT healthcare professionals. This also fortuitously aligned to the political agenda outlined in the NHS Five Year plan published in 2014 [1].
The working system is broadly based on the partnership model of general practice: family doctors who work efficiently and effectively in automatous partnership, sharing clinical knowledge, business acumen and perspective, thus allowing space for individuals to be the best version of themselves with patients.
It is thought that 10-20% of primary care consultations are ENT related [2], which makes the extended role primary care clinician a good gatekeeper to receive and triage referrals. The majority of referrals often follow a predictable clinical pattern, which can lead to fairly consistent investigative and management protocols. This method of approach often follows traditional surgical specialty training. It is therefore our aspiration to upskill clinicians with transferrable skills, whether it be the holistic patient-based communication of the GP, the correct use of audiology equipment and pragmatic understanding of deafness from the audiologist’s perspective, the vestibular exam and subsequent interpretation from the vestibular physiotherapist, the organisation, infection control and patient advocacy of the nurse or, of course, the consultant’s attention to detail, safety netting and perspective.
“It is thought that 10-20% of primary care consultations are ENT related, which makes the extended role primary care clinician a good gatekeeper to receive and triage referrals”
The result is a team of clinical practitioners, highly proficient in their own traditional field and trained to practise in a wider role, within competencies and appropriate support. The benefit of this approach is to give a greater service resource for common presentations, as well as giving accepted clinical advice and perspectives born of their specialist training. We feel this allows for an extra dimension when triaging into and between clinicians.
RELATED TOPIC - Tap the box below
The most obvious transferrable technical skill that can be taught with time, care and effort is microsuction or aural care. Running a microsuction clinic in tandem to a general ENT and hearing aid clinic is seen as important to increase footfall through a clinic session and potentially prevent patients from rebooking and wasting clinic time. Conversely, having an audiology/general ENT clinic bolted onto a microsuction clinic, will soak up the patients who attend aural care with no outer ear disease and require a rapid assessment safety net for presentations such as sensorineural hearing loss, unilateral tinnitus from presumed wax, middle ear disease or associated pathology from the pharynx, postnasal space or cervical spine/TMJ.
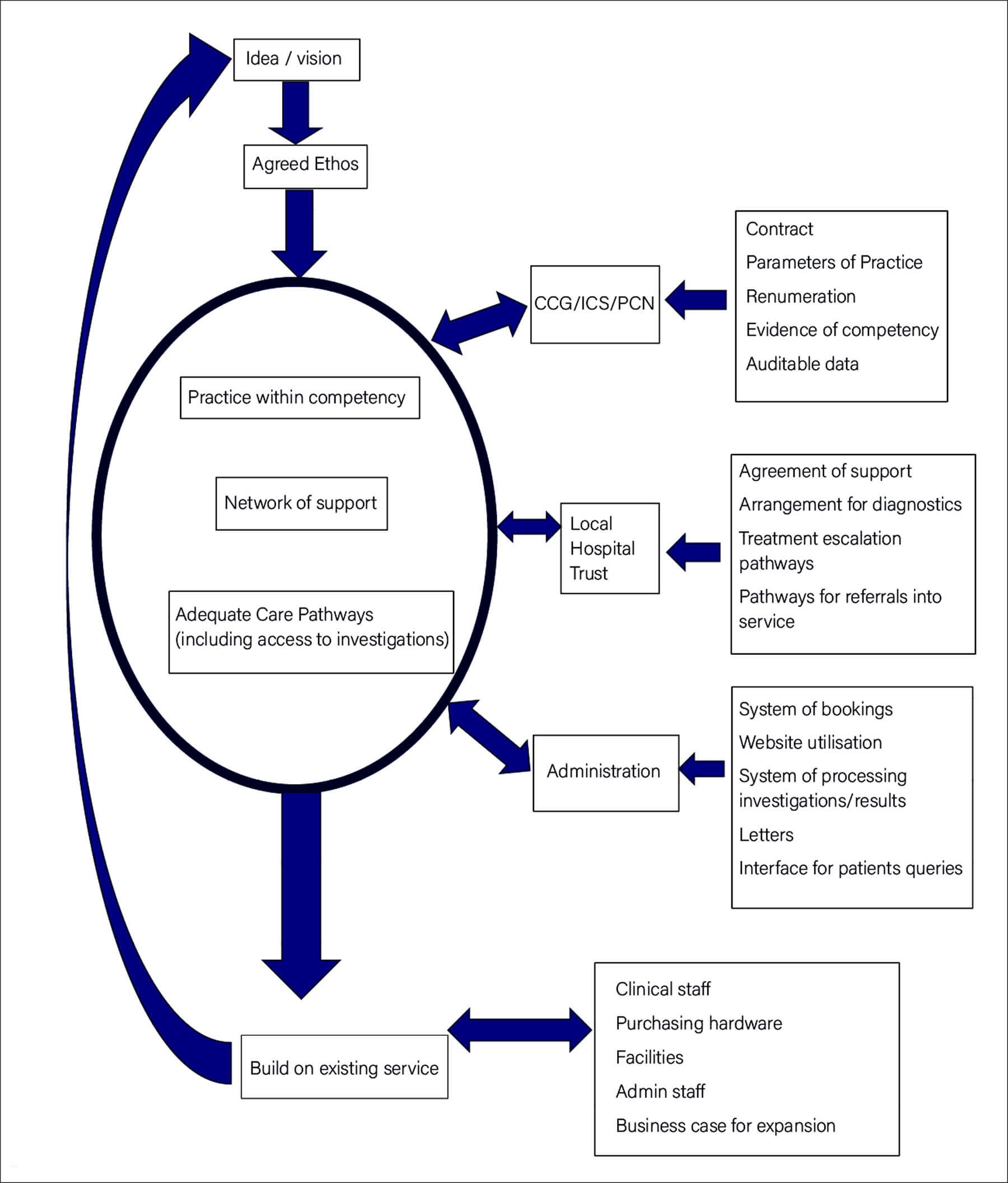
The rise and fall of any service is with its administrative support. Adequate investment in staff to take bookings, write letters, invoice and field patient queries on the phone, must not be underestimated as more clinical staff are brought in.
Another difficult area is bureaucracy: this can insidiously appear in many forms, whether it is related to the processes for CQC or information/clinical governance. It can appear when coordinating pathways or systems involving the CCG/ICS or local trusts. One cannot overstate the glacial nature of devising and implementing a pathway in the NHS. Relationships with the right individuals can often take years to cultivate and depend on trust and honesty.
“The benefit of this approach is to give a greater service resource for common presentations, as well as giving accepted clinical advice and perspectives born of their specialist training”
However, healthcare requires clinicians at its core and our ethos is to bring them in whenever possible and build a service around their core skill set and, in the process, slowly break down the antiquated egoic Royal College hierarchies. It fundamentally depends on individuals to bring their authentic selves to work and the community to move together to achieve desired outcomes. Unfortunately, pay is not a motivating factor in the NHS to keep clinicians in post but, surprisingly, we are able to draw clinician’s out of the private sector. The financial lure is countered by exposure to varied and interesting pathology, getting support from the different specialists when needed, working to family-friendly hours and having the opportunity to learn different skills if desired. The flip side to this culture of working is that it does require the ability to be clinically flexible, to have personal ownership over the patient journey through the service and hold responsibility for the preparation and tidying of clinical spaces. Having regular governance meetings, which include space to meet continuing professional development needs, also serves as a platform to raise fears, worries and areas of conflict. All voices, from admin to consultant, are regarded with equal weight around these figurative ‘round table’ meetings, promoting individuals to be heard and learning to occur, with the desired effect to remove toxic stress from the workplace and develop vocational satisfaction.
References
1. NHS Five Year Forward View. 2014.
www.england.nhs.uk/publication/
nhs-five-year-forward-view
Last accessed January 2022.
2. Griffiths E. Incidence of ENT Problems in General Practice. J R Soc Med 1979;72(10):740-2.
Declaration of competing interest: Sudeb Mandal is part of a team of clinician’s who run the Kent Community ENT service, which is contracted by the NHS. No private work is done.






