Raewyn Campbell is a rhinologist and skull base surgeon in Sydney, Australia. Prior to training in medicine, she was trained as a physiotherapist, and she brings both disciplines into her research on ergonomics in surgery. Surgeons need to look after themselves as well as their patients. Raewyn will be addressing this in person in Dublin but, here, she gives you a flavour of what she will be talking about.
Surgery is hurting surgeons, and it is doing so at an increasing rate. Work-related musculoskeletal disorders (WRMD) are the largest occupational health and safety problem in many countries [1]. WRMD are broadly categorised into biomechanical hazards and psychosocial hazards.
The two key identified factors contributing to the continued high prevalence of WRMD are shortcomings in the implementation of effective ergonomic practices and the failure to include psychosocial risks in risk assessments [2]. Ergonomics is a science that studies workplaces with the aim to optimise the interaction between the worker, equipment, task and the environment. The aims of ergonomics are to minimise injury whilst also maximising efficiency. Psychosocial hazards include factors such as work demands, organisational support and interpersonal work relationships.
"Up to 90-100% of surgeons have regular work-related musculoskeletal pain, which commonly first develops during training"
Due to the rise and overwhelming negative impact of WRMD on disability and absenteeism, ergonomics has been successfully embraced in many industries including mining, construction and in the military. Whilst WRMD in these industries are now decreasing, the healthcare industry has some of the highest rates. Unfortunately, the rates of WRMD in healthcare are increasing, particularly in surgeons [3,4]. Surgical ergonomics has received relatively little attention to date, despite this population being at particularly high risk for WRMD. Up to 90-100% of surgeons have regular work-related musculoskeletal pain, which commonly first develops during training [4]. Otorhinolaryngologists have some of the highest rates of WRMD among the surgical subspecialties, and the impact can be significant. Surgeons with WRMD have lower job satisfaction, higher rates of burnout, are more callous towards people and are more likely to retire earlier than planned [5]. Work-related musculoskeletal disorders also negatively impact a surgeon’s performance which can result in worse outcomes for our patients.
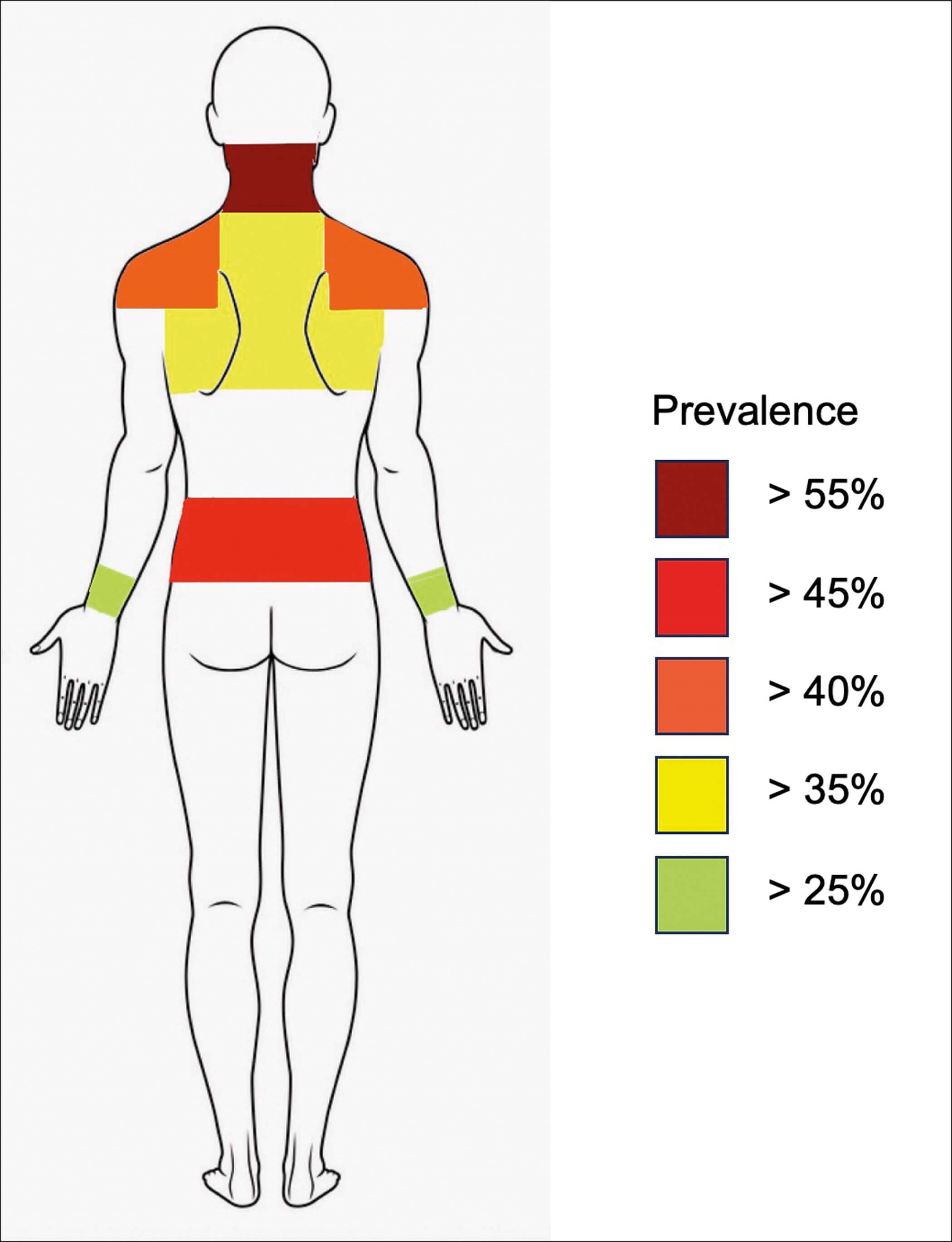
Figure 1: Body map of WRMSDs prevalence by body area in otorhinolaryngologists.
Author’s own data.
Common areas of WRMD in otorhinolaryngology
Most commonly, otorhinolaryngologists experience the most significant musculoskeletal symptoms in the shoulders, neck and lower back (Figure 1). Our work-related musculoskeletal pain usually starts during surgery but does not peak until after we finish operating. The symptoms do not return to baseline for two to three days, if we are permitted to rest from work during that time.
The problem with surgical ergonomics to date
Very few surgeons have received appropriate and effective ergonomics training. Further, our index of safety has focused on patient morbidity and mortality with no analysis of surgeon morbidity. Healthcare ergonomics has also traditionally centred on occupational health and safety, which has involved manual handling training and postural screening. Yet, manual handling training and postural screening have been found to be ineffective in reducing back pain and injury. In fact, back pain is not purely restricted to occupations that involve lifting and carrying heavy loads. In surgery, it is the combination of prolonged, awkward postures and repetitive movements using one size fits all instrumentation and wearing inappropriate equipment and clothing, all whilst performing a cognitive task in a poorly designed operating room that contributes to our WRMD.
Myths about ergonomics
Many outdated beliefs persist in the medical profession about ergonomic principles. These include: the benefits (or lack thereof) of a neutral body posture, lifting weight limits, the avoidance of lifting with a flexed lumbar spine, the avoidance of a slouched sitting posture, the benefits of current manual handling practices and current exercise recommendations. These, and many other beliefs now need to be revisited in light of current research.
What can we do to reduce our WRMD?
There are many barriers to developing programmess to prevent WRMD. The research into strategies to reduce WRMD in otorhinolaryngology is sparse but increasing. However, there are many strategies to reduce our WRMD. Firstly, we need to promote awareness and the need for intervention in this area and involve end-users in communication and strategy development. Secondly, we need more and higher quality research in the field of surgical ergonomics. The development of surgery-specific risk assessment tools that incorporate both the physical and psychosocial hazards will benefit surgical ergonomics greatly. Finally, we need to incorporate ergonomics into surgical training and education at a very early stage, and to continue this training throughout our careers.
"The development of surgery-specific risk assessment tools that incorporate both the physical and psychosocial hazards will benefit surgical ergonomics greatly"
However, surgeons can institute simple changes immediately to reduce their WRMD. These include changes in the following areas: learning how to identify musculoskeletal risks early and intervening appropriately; choice of footwear; ordering your surgical list to minimise injury; posture whilst operating; type, intensity and frequency of exercise and fitness; operating room set-up and design; equipment choice and placement; dietary choices; the type of loupes and headlights used and how to use them; choice of operating room chair; table height; patient positioning; ergonomic mentorship to name a few.
In summary, WRMD are common and increasing in our profession. There are many reasons for these injuries, however, many are within our ability to change. We can no longer regard WRMD as part of the job and we must become increasingly aware of the negative impact they have on us, our colleagues and our patients. This will be the first step to addressing this increasingly significant health problem and to improving outcomes for ourselves, our colleagues and our patients.
References
1. De Kok J, Vroonhof P, Snijders J, et al. Work-related MSDs: prevalence, costs and demographics in the EU. European Agency for Safety and Health at Work. 2019.
2. Crawford J, Davis A. Work-related musculoskeletal disorders: why are they still so prevalent? Evidence from a literature review. 2020.
3. HSE. Health and safety at work: Summary statistics for Great Britain 2023.
www.hse.gov.uk/statistics/assets/
docs/hssh2223.pdf
[Last accessed November 2023]
4. Epstein S, Sparer EH, Tran BN, et al. Prevalence of work-related musculoskeletal disorders among surgeons and interventionalists. JAMA Surgery 2018;153(2):e174947.
5. Wells AC, Kjellman M, Harper SJF, et al. Operating hurts: a study of EAES surgeons. Surg Endosc 2019;33:933-40.
Declaration of competing interests: None declared.







