Why laryngotracheal stenosis and malacia (LTSM) care matters now?
In late 2019, reports began to emerge of severe respiratory infections caused by a novel coronavirus. In the months that followed, intensive care admissions in the UK rose more than tenfold. At the time, we and others predicted that the rise in Covid-related intubations would be followed by a disproportionate rise in intubation-related laryngotracheal stenoses [1]. In the event, the increase was real but much smaller than expected.
The blunted rise in the incidence of laryngotracheal stenosis owes much to our intensive care colleagues who, at great personal cost and under the immense strain of uncertainty, maintained an extraordinary quality of patient care. The rise in the incidence of LTSM (Figure 1) is likely to reflect a combination of a genuine increase in cases, a rise in a different type of airway disease (excessive dynamic airway collapse; EDAC), and improved recognition of LTSM leading to the detection of more cases.
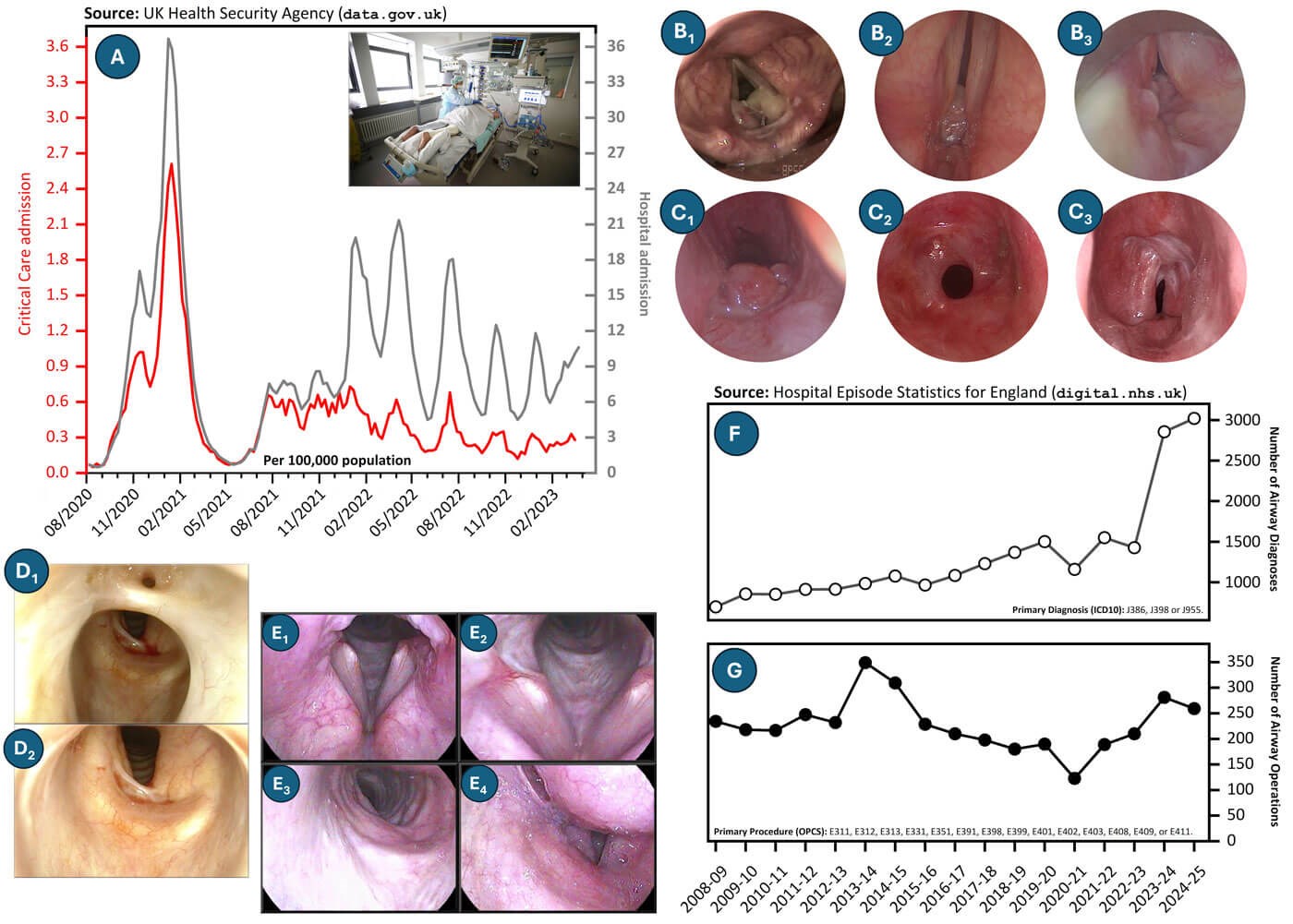
Figure 1: A. The impact of the Covid-19 pandemic on hospital and critical care admissions in the UK; B1–3. Different patterns of acute laryngeal injuries associated with Covid-19; C1-3. Different patterns of tracheal injury associated with Covid-19. D1–2. Two-level (posterior commissure and A-frame tracheal) stenosis following Covid-19 infection; E1. Glottic inlet at maximum-effort inspiration during transnasal tracheoscopy. Laryngeal abduction is reduced. This is not due to restricted abduction, but to air escape due to the presence of laryngeal diastasis; E2. Laryngeal diastasis is more clearly visible and the patient demonstrates paradoxical expiratory abduction; E3. Proximal trachea during maximum-effort inspiration; E4. Proximal trachea during maximum-effort expiration, demonstrating tracheostomy-related airway malacia; F. The number of hospital admissions with primary diagnoses of LTSM between 2008 and 2025; G. Number of hospital admissions for LTSM primary procedures over the same period.
What is LTSM?
LTSM is an umbrella term for different conditions that cause exertional dyspnoea due to narrowing or instability of the supraglottic, glottic, subglottic, tracheal and/or main bronchial airways. In adults, the most common cause remains endotracheal intubation and mechanical ventilation.
Bilateral vocal fold immobility can result from intubation-related laryngeal fixation, either through posterior glottic scarring or cricoarytenoid joint ankylosis. It may also result from bilateral recurrent laryngeal nerve injury or, less commonly, neuromuscular weakness (e.g. myasthenia gravis). Cricoarytenoid joint ankylosis may also occur in rheumatoid arthritis. Inflammatory and non-malignant infiltrative processes, including sarcoidosis, amyloidosis, IgG4-related airway disease and idiopathic subglottic stenosis cause submucosal deposition with progressive airway narrowing. By contrast, granulomatosis with polyangiitis and tuberculosis cause mucosal necrosis with cicatrix formation due to secondary wound-healing [2].
Large-airway collapse syndrome arises from loss of cartilaginous support (tracheobronchomalacia), or from excessive invagination of the posterior tracheal wall due to neuromuscular discoordination (EDAC) [3]. Relapsing polychondritis is especially challenging because it can produce both stenosed and malacic segments [4].
A small number of paediatric airway problems continue to require management in adulthood. LTSM does not include obstructive sleep apnoea, airway obstruction caused by deep-space head and neck infection, or obstruction due to malignancy such as head and neck or tracheal squamous cell carcinoma, lung cancer, or thyroid, thymic and oesophageal tumours compressing or invading the airway. However, highly selected malignancies such as low-grade chondrosarcoma or adenoid cystic carcinoma may present choices that overlap with LTSM practice and require laryngotracheal diagnostic, surgical and rehabilitative skills in a multidisciplinary context [2].
When should LTSM be suspected?
LTSM is a rare cause of exertional dyspnoea. For every newly-diagnosed case of adult intubation-related laryngotracheal stenosis, 837 patients are given a new diagnosis of adult-onset asthma that same year [5,6]. There are, however, a few faint zebra stripes on the back of the horse that should create an index of clinical suspicion for LTSM.
The clearest cases of symptoms suggestive of LTSM are breathlessness with stridor, tracheal tug, supraclavicular recession or other signs of upper airway obstruction. Failed extubation, or new or worsening exertional dyspnoea developing within weeks to a few months of extubation or tracheostomy decannulation, should be considered laryngotracheal until proven otherwise [7]. New-onset dyspnoea in a patient with granulomatosis with polyangiitis (GPA) should also be assumed to have a laryngotracheal origin; recurrent chest infections in the same context should raise suspicion of bronchial involvement [8].
Airway stenosis in granulomatosis with polyangiitis is predictably unpredictable. It may evolve while systemic disease appears quiescent and inflammatory markers are reassuring [9]. Breathlessness may precede abnormalities in blood tests, standard lung function tests or CT imaging. Airway symptoms should not be dismissed as deconditioning, asthma, anxiety or non-specific breathlessness until laryngotracheal and bronchial disease have been excluded. This problem is treatable if recognised early, yet bronchial stenosis is still diagnosed too late.
Suspicion should also be maintained in patients with relapsing polychondritis, sarcoidosis, amyloidosis, IgG4-related disease, rheumatoid arthritis, previous airway surgery or neck radiotherapy. Patients labelled as having idiopathic subglottic stenosis should be reconsidered if the demographics are atypical, the airway looks unusually inflamed, or repeated dilations are required at intervals shorter than six months. A diagnosis of difficult or adult-onset asthma should not be considered secure in pregnant women until idiopathic subglottic stenosis has been actively excluded [10].
What about the ‘incidental’ stenosis?
Computed tomography (CT) is often obtained in patients with unexplained dyspnoea. It may identify upper airway narrowing. However, CT scans have significant false-positive and false-negative rates for laryngotracheal problems, and their findings should strongly raise suspicion and not be regarded as definitively diagnostic [11]. We agree with recently published guidance on managing laryngotracheal stenosis that recommends direct visualisation as the diagnostic standard [12].
What should be done with a newly diagnosed case?
Acute management of respiratory compromise attributable to LTSM follows standard ABCD principles. These patients will, by definition, have difficult airways and the Difficult Airway Society guidance should therefore be carefully followed when managing them [13]. In our experience, performing rigid or sedated bronchoscopy for acute proximal airway obstruction can be hazardous. If a tracheostomy is the only available life-saving option, it must be performed without delay or hesitation. Unless a subspecialist laryngotracheal surgeon is available, a tracheostomy should be what is performed without delay or hesitation. The patient should then be transferred to the airway unit.
Chronically breathless but stable patients should be referred to a subspecialist LTSM clinic when the history is compatible with LTSM, and flow-volume loops, CT imaging or endoscopy support the diagnosis. Patients with non-healing tracheocutaneous fistulae after decannulation, or long-term tracheostomy dependence with suspected LTSM, should be referred to the LTSM clinic urgently.
What is a subspecialist LTSM clinic?
This clinic offers one-stop diagnostic assessment, treatment planning, holistic support and follow-up for patients with known or strongly suspected LTSM (Appendix 1). This condition, even when restricted to the trachea, is seldom a single-organ disease. Most patients have breathing, voice, throat, swallowing, cough, secretion-control, deconditioning, autonomic and psychological morbidity.
The team is led by a laryngologist whose primary superspecialty focus is LTSM, working as part of a wider multidisciplinary team that includes airway speech and language therapists (ASLTs), airway clinical nurse specialists, respiratory physiologists, rheumatologists, respiratory physicians and subspecialist anaesthetists. There are close links to thoracic surgery, rehabilitation medicine and critical care. One gap in our current offering is dependable access to clinical psychology.
Speech and language therapists are central to the LTSM clinic, providing joint assessment and treatment for breathing pattern disorders, voice disorders, cough, secretion management, swallowing and aspiration, and working with psychology colleagues to support patients’ psychological adjustment, resilience and recovery from the impact of chronic disease and critical illness. Joint assessment and explanation of airway anatomy, disease behaviour, treatment options and warning symptoms are often reinforced in follow-up consultations, which may also include SLT-led stroboscopy to guide therapy and instrumental swallowing assessment, providing patients with a framework for empowered self-management. SLTs also provide the point of contact for tracheostomy-free patients. The airway nurse specialists share this activity and take a leading role in supporting patients with tracheostomies.
What do we assess in our LTSM clinic?
All first-time assessments include the integrated foregut clinical history [14]. If vasculitis is suspected, the Birmingham Vasculitis Activity Score is also documented [15]. The laryngologist and ASLT jointly assess breathing effort, breathing pattern, voice, cough, secretion control, dysphagia, swallowing safety and throat function. Clinical assessments are supplemented by electroglottography (Appendix 2), 100 ml timed water-swallow test, flow-volume loops and validated patient-reported outcome measures (Appendix 3).

Figure 2: Laryngostroboscopy (already performed) and proximal tracheoscopy (being performed). Image produced with patient’s written permission for publication of identifiable media.
Patients undergo laryngostroboscopy and proximal tracheoscopy. Through specific anaesthetic techniques (the three-pass method), enhanced manoeuvres to expose the subglottis [16] and mindful endoscopy [17], the proximal trachea can be examined in approximately 95% of patients in the clinic with good patient experience (Figure 2). Patient experience is measured using a validated patient-reported experience measure. General findings such as mucosal inflammation, pooling of secretions, and vocal fold mobility and vibration observed during laryngoscopy and proximal tracheoscopy also define the site, extent and character of more proximal stenoses. Large-airway collapse is screened for by observing for paradoxical expiratory abduction on maximum-effort breathing [3]. Flow-volume loops provide visual and objective measures of flow-limitation, and the laryngologist-ASLT assessment identifies general and stenosis-specific breathing pattern problems. Together, these constitute the outpatient triple airway assessment.
What is assessed after the LTSM clinic?
Further investigations are selected on a case-by-case basis. Blood tests are requested with rheumatology input when the boundary between idiopathic, inflammatory and immune-mediated stenosis is unclear. ANCA testing is helpful, but not definitive.
Transnasal panendoscopy is used for selected patients with dysphagia or recalcitrant throat symptoms [18]. Transnasal tracheoscopy, better described as a lip-to-bronchus assessment, is performed as part of the triple assessment of suspected tracheomalacia or EDAC, alongside airway-focused cardiopulmonary exercise testing and response to a titrated CPAP trial. Transnasal tracheoscopy is also used to assess more distal stenoses and for surveillance of patients with idiopathic or vasculitis-associated laryngotracheal stenosis [19]. Fibreoptic endoscopic evaluation of swallowing, videofluoroscopy and oesophageal function testing are used when swallowing and reflux morbidity may influence treatment.
Examination under anaesthesia (EUA) is indicated in two specific circumstances: when a patient with posterior glottic stenosis is being considered for open surgery, where EUA via suspension laryngotracheoscopy (Appendix 1) allows assessment of cricoarytenoid joint mobility, posterior commissure scarring, and concurrent tracheal disease; and when tracheal or cricotracheal resection is being considered, where EUA with suspension laryngotracheoscopy and magnified mucosal chromoendoscopy enables precise assessment of airway dimensions and submucosal disease extension, which may alter the planned resection length, preclude open surgery, or necessitate additional release manoeuvres. In these two specific scenarios and in the very small number of patients who cannot have awake airway assessments, EUA is performed instead of transnasal tracheoscopy/conventional bronchoscopy, to guide the plan.
Our philosophy of managing LTSM is to establish a precise diagnosis and to match the full range of treatment to the diagnosis in the context of underlying morbidities and patient expectations. At the same time, the patient is holistically supported to reduce symptoms and morbidity across all of the systems and functions that LTSM affects.
How is LTSM treated?
Treatment should be mechanism-based, not diameter-based. A short, stable stenosis, an inflamed recurrent cicatrix, posterior glottic fixation, neuromuscular discoordination, laryngeal myasthenia gravis and dynamic airway collapse may all produce exertional dyspnoea, but they are different diseases and require different treatments.
Not every patient needs an operation. Many patients with EDAC, and some with tracheobronchomalacia, can be treated with CPAP, weight-loss support, pulmonary rehabilitation and breathing-pattern therapy. CPAP is both a diagnostic test and a therapeutic pneumatic splint: improvement during a titrated trial helps identify patients whose symptoms are driven by dynamic collapse and who may benefit from longer-term non-surgical management or from surgical intervention if their daytime symptoms remain disabling.
Speech and language therapists provide joint assessment as well as primary and adjunctive treatments. Highly specialist ASLTs support breathing-pattern retraining, breath support for voice, cough control, secretion clearance, hydration, airway surface health and reduction of laryngeal irritants. In patients with LTSM, breathlessness can persist following treatment, not because the airway is still narrow, but because of entrenched breathing patterns, which ASLT helps patients overcome. Postoperative therapy helps patients recalibrate their breathing pattern after the airway has changed, rebuild confidence in exertion and avoid the cycle of dyspnoea, panic, throat tightening and further breathlessness. ASLT ongoing management prevents the patient’s breathing pattern from snapping back to the pre-treatment state.
Minimally invasive surgery is what guidelines recommend as first-line approach to LTSM [20]. For idiopathic, vasculitis-associated and selected post-intubation laryngotracheal stenoses, endoscopic laryngotracheoplasty is our main procedure. This is not an incision and dilation with or without steroids or mitomycin C [21]. Its aim is to remodel the stenotic segment in a way that reduces early recurrence, but without precipitating aggressive disease recurrence through over-resection. We are very cautious about using balloons across the glottis and subglottis, due to the risk of proximal stenosis migration leading to laryngeal fixation [21]. An idiopathic or vasculitis-related laryngotracheal stenosis, once converted into an iatrogenic glottic-subglottic-tracheal stenosis, becomes an exceptionally difficult condition to manage [22]. For A-frame post-tracheostomy stenosis, endoscopic tracheal resection is the first-line procedure [23]. It achieves the same outcome as an open resection in >90% of cases without risking anastomosis dehiscence or vocal palsy, and without compromising the possibility of future open surgery, if needed. All of these procedures are enabled through translaryngeal shared-airway microsurgery techniques, which in turn require clear planning and communication using a common language, with team skills maintained through deliberate practice. To enable this, we have created a standard operating procedure that defines patient flow before, during and after surgery (Appendix 4).
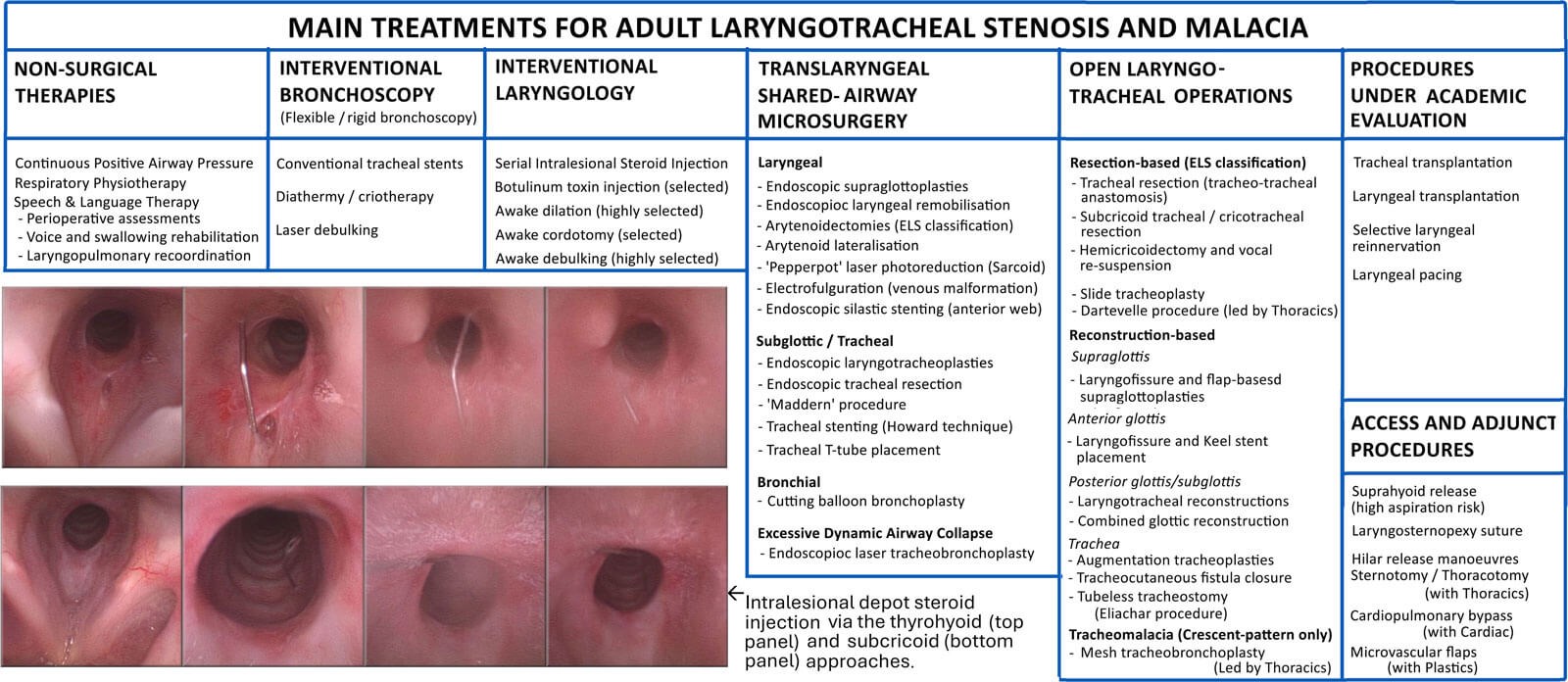
Figure 3: Different treatments for adult laryngotracheal stenosis and malacia. The inset shows intralesional steroid injection performed via the cricothyroid (top panel) and retrograde (bottom panel) technique.
Serial intralesional steroid injections (Figure 3) have allowed “serial regression of lesion” to be achieved without the need for multiple general anaesthetics (Figure 3) [24,25]. Analogous to treating keloidal-type scarring elsewhere, serial steroid injections suppress inflammatory scar activity to prolong the interval between operative procedures. More importantly, they reduce the likelihood that the patient’s airway becomes compromised between treatments again. This is especially important to prevent a relapsing remitting course of breathing unreliability, pre-treatment distress and physical and psychological morbidity. In this setting, maintenance treatment is proactive rather than reactive: patients are followed clinically, endoscopically and physiologically (the triple airway assessment protocol) so that recurrence is treated before its symptoms become distressing and debilitating again.
Bilateral vocal fold immobility and high subglottic stenoses require a different treatment logic because airway, voice, swallowing and airway protection are competing priorities at the posterior glottis. Options include observation, temporary procedures such as lateralisation suture to avoid tracheostomy, tracheostomy in highly selected cases, scar division and arytenoidectomy. With laryngeal stenosis, every option is a trade-off and this should be made clear as part of obtaining informed consent. For this reason, the European Laryngological Society has provided a subclassification of arytenoidectomies to enable surgeons to match the exact obstruction pattern to the subtly but clinically distinct treatments that have been developed (Figure 4) [26].
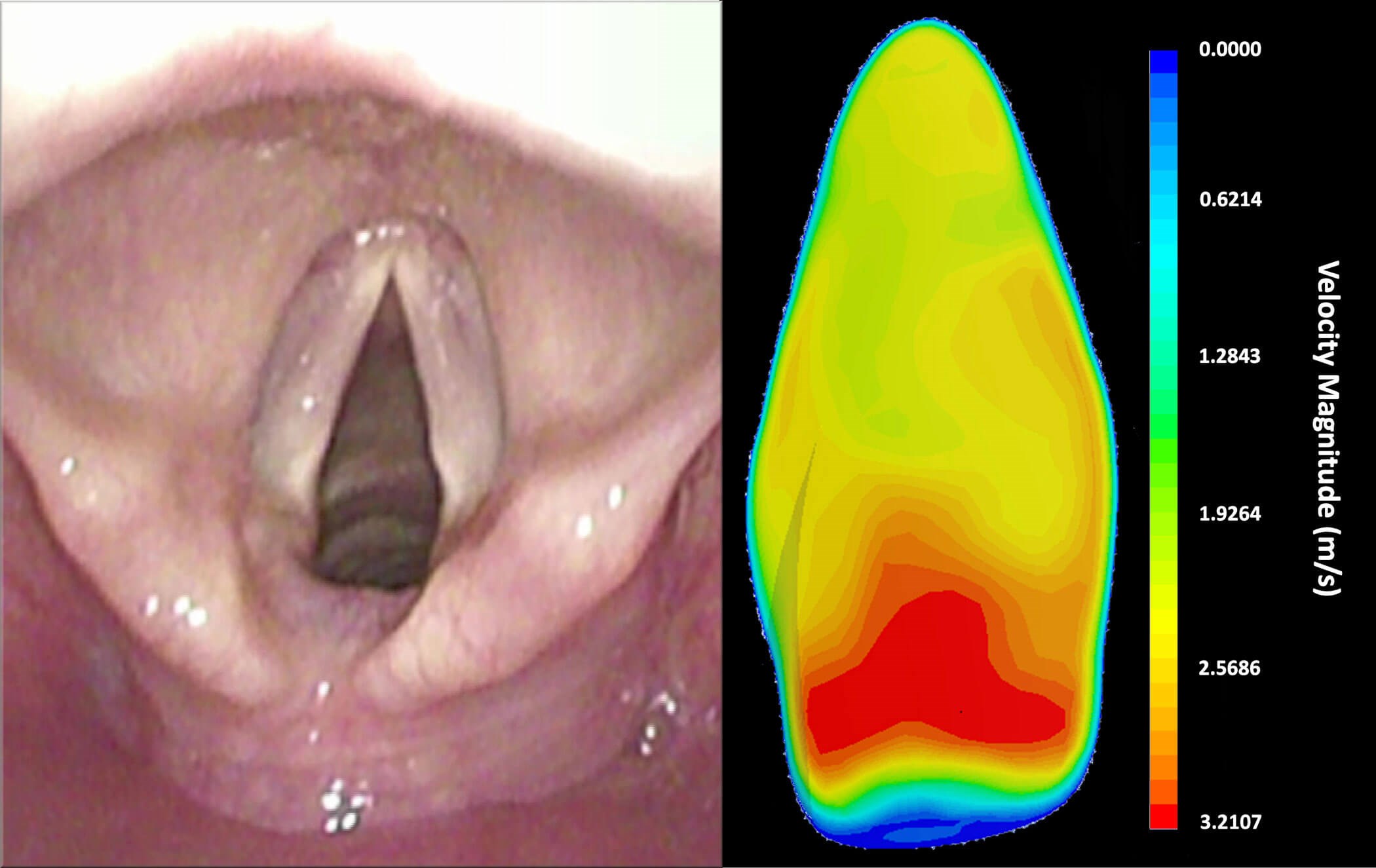
Figure 4: Laryngeal inlet (left) and computational fluid dynamic modelling of airflow through the glottis (CFD image provided courtesy of Professor Dennis Doorly, Imperial College London).
Systemic treatments have an expanding role [27]. Procedural treatment can restore airway calibre, but it does not always address the biological driver. In GPA, IgG4-related disease and relapsing polychondritis, immunomodulatory treatment may complement procedural intervention by suppressing the inflammation that drives recurrence. Rituximab is part of standard care for selected patients with active GPA and IgG4-related disease. It is not routine treatment for idiopathic subglottic stenosis, but has been used in highly selected patients with aggressively recurrent airway disease after multidisciplinary review, especially when there is diagnostic overlap or uncertainty with ANCA negative GPA [28].
Airway stents are not routine long-term treatments for benign LTSM. They can migrate, crust, provoke granulation tissue and impair mucociliary clearance. Standard wall-gripping stents are effective in relieving symptoms of malignant airway obstruction, often in end-of-life settings. They cause major complications when used to treat benign disease and should be altogether avoided in that setting [29[. Long-term stenting, using the Howard technique, is an option in highly selected cases [3].
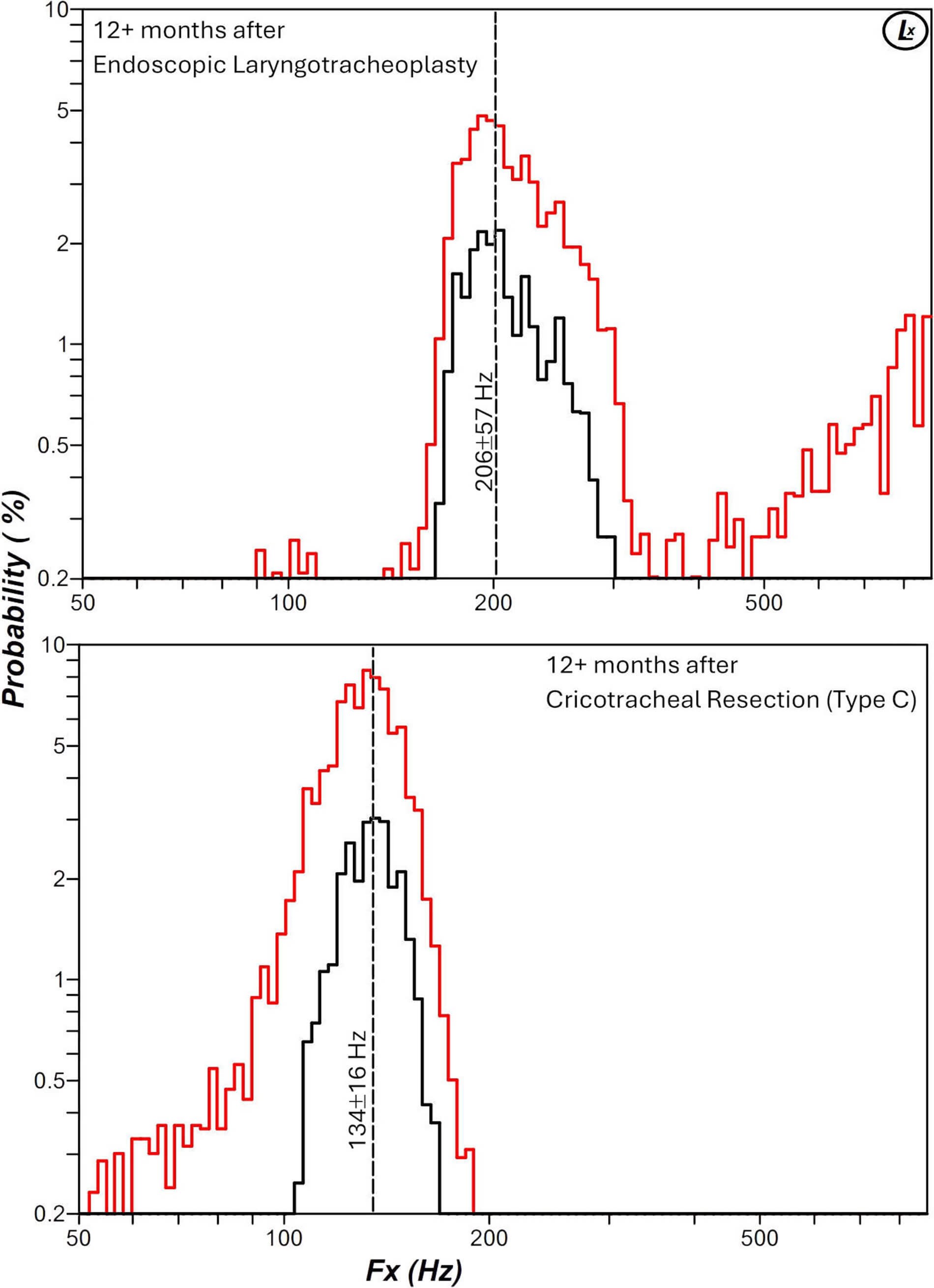
Figure 5: Frequency electroglottography plots of a patient following endoscopic laryngotracheoplasty and serial intralesional steroid injection (top graph) and following cricotracheal resection (bottom panel), the latter showing significant impact and morbidity on the female voice. Full electroglottography of these patients are provided in Appendix 2. These demonstrate the trade-offs in managing LTSM. A cricotracheal resection can achieve long-term disease remission in 90% of patients but it carries significant risks, including death due to anastomosis dehiscence. It is also associated with permanent voice morbidity. The Maddern procedure can also achieve long-term disease remission, but it too is associated with significant risks including tracheosophageal fistula formation and long-term refractory cough and mucous. Serial dilations require fewer visits to hospital but are associated with prolonged periods, as the stenosis begins to reform but before it is sufficiently advanced to justify the next surgery, where the patient experiences significant physical and psychological morbidity. Endoscopic laryngotracheoplasty and postoperative serial intralesional steroid injections enable prolonged symptom-free periods and minimise the number of general anaesthetics, but they are associated with more visits to the hospital and the interventional laryngology unit to maintain the airway. Some patients also experience side-effects from steroid injection. All options have advantages and trade-offs and the ability to offer all options to avoid biasing patient choices toward a subset of treatments, and remaining vigilant to patient preferences, which may change over time, is key to offering patient-centred care.
Open surgery (laryngotracheal reconstruction and tracheal/cricotracheal resection) remains necessary for a diminishing number of patients. If the first principle of surgical management for LTSM is to favour minimally-invasive surgery over open surgery (to avoid the added morbidity and cost of open surgery), the second consideration is to favour airway augmentation over segmental resection (to avoid the risks of anastomosis dehiscence and suture-line re-stenosis) [30]. Open airway operations are effective in improving airway calibre, but they alter voice (Figure 5) and may alter swallowing, cough, airway sensation and future airway access, often to a greater degree and at considerably greater healthcare cost than their minimally-invasive alternatives. No patient should be considered for open surgery until minimally invasive and less risky open alternatives have been discussed with them in the LTSM clinic. At our unit, all patients undergoing open surgery have standardised surgical approaches and receive highly structured postoperative care using the ‘enhanced recovery after surgery’ approach (Appendix 5).
Future directions
The future of LTSM care is precise personalisation. Patients have traditionally been grouped by anatomy and their treatment decided on by the specific skillsets of surgeons. A more useful classification combines anatomy, physiology, inflammatory activity, scar biology, comorbidity and patient priorities.
Disease-modifying medical treatment for fibrosis remains a major unmet need. Current treatments can divide, dilate, inject, resect or reconstruct scars, but they do not reliably alter the biology that produces recurrent cicatrices. Whereas not too many years ago, low-volume high-pressure endotracheal tubes produced severe injuries due to isachemic necrosis of the larynx and trachea but with normal intrinsic wound-healing responses, now LTSM is primarily a sequala of abnormal wound-healing. Better understanding of fibroblast behaviour, epithelial injury and aberrant wound healing may move treatment beyond repeated mechanical correction.
Laryngeal pacing is another important frontier. Current glottic-widening operations for bilateral vocal fold paralysis improve breathing by sacrificing some element of voice, cough or swallow protection. While this morbidity can be minimised by precise planning and SALT-led rehabilitation, a treatment that reliably restores inspiratory abduction while preserving laryngeal structure would represent a paradigm shift in care.
By contrast, tracheal replacement remains elusive. Despite decades of effort, no substitute yet reproduces the structural strength, epithelial function, vascularity, mucociliary clearance, infection resistance and growth potential of the native airway. For now, progress is more likely to come from prevention, earlier recognition, precise surgery, stronger rehabilitation and medical treatments that make recurrent fibrosis less inevitable.
References
1. Piazza C, Filauro M, Dikkers FG, et al. Long-term intubation and high rate of tracheostomy in COVID-19 patients might determine an unprecedented increase of airway stenoses: a call to action from the European Laryngological Society. Eur Arch Otorhinolaryngol 2021;278(1):1–7.
2. Sandhu GS, Nouraei SAR. Laryngeal and Tracheobronchial Stenosis. San Diego, CA, USA; Plural Publishing: 2016.
3. Girgis M, Nouraei S. Treating life-threatening airway compromise due to concurrent COPD and tracheomalacia using translaryngeal shared-airway microsurgery. Ann R Coll Surg Engl 2026 [ePub ahead of print].
4. Maciazek-Chyra B, Szmyrka M, Skoczynska M. Relapsing polychondritis - analysis of symptoms and criteria. Reumatologia 2019;57(1):8–18.
5. Nouraei SA, Ma E, Patel A, et al. Estimating the population incidence of adult post-intubation laryngotracheal stenosis. Clin Otolaryngol 2007;32(5):411–2.
6. Eagan TM, Brogger JC, Eide GE, Bakke PS. The incidence of adult asthma: a review. Int J Tuberc Lung Dis 2005;9(6):603–12.
7. Gulilat D, Genetu A, Kejela S, et al. Nonmalignant tracheal stenosis: presentation, management and outcome in limited resources setting. J Cardiothorac Surg 2024;19(1):21.
8. Nouraei SA, Mills H, Butler CR, et al. Outcome of treating airway compromise due to bronchial stenosis with intralesional corticosteroids and cutting-balloon bronchoplasty. Otolaryngol Head Neck Surg 2011;145(4):623–7.
9. Nouraei SA, Obholzer R, Ind PW, et al. Results of endoscopic surgery and intralesional steroid therapy for airway compromise due to tracheobronchial Wegener’s granulomatosis. Thorax 2008;63(1):49–52.
10. Barbera JP, Mossayebi MH, Khanuja K, et al. Idiopathic subglottic stenosis in pregnancy: A systematic review. Int J Gynaecol Obstet 2026;173(2):674–85.
11. Corcoran A, Foran A, Phinizy P, et al. Dynamic airway computed tomography and flexible bronchoscopy for diagnosis of tracheomalacia in children: A comparison study. Pediatr Pulmonol 2024;59(4):899–906.
12. Norwood S, Vallina VL, Short K, et al. Incidence of tracheal stenosis and other late complications after percutaneous tracheostomy. Ann Surg 2000;232(2):233–41.
13. Ahmad I, El-Boghdadly K, Iliff H, et al. Difficult Airway Society 2025 guidelines for management of unanticipated difficult tracheal intubation in adults. Br J Anaesth 2025;136(1):283–307.
14. Parkes R, Probert C, Baker S, et al. The Integrated Foregut Clinical History: enabling nurse-led, joined-up initiation of suspected-cancer pathways. Br J Nursing 2026;35(6):328–37.
15. Luqmani RA, Bacon PA, Moots RJ, et al. Birmingham Vasculitis Activity Score (BVAS) in systemic necrotizing vasculitis. QJM 1994;87(11):671–8.
16. Highland J, Torrecillas V, Redding T, et al. Optimization of Subglottic View During Flexible Laryngoscopy With Patient Positioning. Otolaryngol Head Neck Surg 2023; 169(6):1556–63.
17. Bond J, Jones E, Turner LA, Nourael SR. Mindful endoscopy: holistically supporting patients through awake examinations of the path of swallowing. Br J Nurs 2026;35(1):16–24.
18. Williams EJ, Nouraei SAR. Should twin-mode white-light and virtual chromoendoscopy of pre-defined mucosal stations be considered a standard of care for Transnasal Panendoscopy? Clin Otolaryngol 2021;46(4):915–7.
19. Ring S, Bowen AJ, Griffin T, et al. Bronchial Mucosal Abnormalities in Idiopathic Subglottic Stenosis. Laryngoscope 2026 [ePub ahead of print].
20. Cho JH, Huh G, Cho JK, et al. Guidelines for the Management of Adult Subglottic and Tracheal Stenosis From the Korean Bronchoesophagological Society. Clin Exp Otorhinolaryngol 2026;19(1):1–20.
21. Nouraei SAR, Dorman EB, Johnston J, Vokes DE. Vocal fold fixation due to proximal stenosis progression complicating idiopathic subglottic stenosis. Eur Arch Otorhinolaryngol 2019;276(8):2293–300.
22. Nouraei SA, Sandhu GS. Outcome of a multimodality approach to the management of idiopathic subglottic stenosis. Laryngoscope 2013;123(10):2474–84.
23. Nouraei SA, Sandhu GS. Outcome of endoscopic resection tracheoplasty for treating lambdoid tracheal stomal stenosis. Laryngoscope 2013;123(7):1735–41.
24. Franco RA Jr, Husain I, Reder L, Paddle P. Awake serial intralesional steroid injections without surgery as a novel targeted treatment for idiopathic subglottic stenosis. Laryngoscope 2018;128(3):610–7.
25. Nouraei SA, Singh A, Patel A, et al. Early endoscopic treatment of acute inflammatory airway lesions improves the outcome of postintubation airway stenosis. Laryngoscope 2006;116(8):1417–21.
26. Dronkers EAC, Al Yaghchi C, Lechien JR, et al. European consensus on endoscopic surgery for bilateral vocal fold immobility: classification and nomenclature. Eur Arch Otorhinolaryngol 2025;282(2):937–44.
27. Torres SJ, Neevel AJ, Ford JA, et al. Immunosuppression and Surgery-Free Interval in Granulomatosis With Polyangiitis Airway Stenosis. Laryngoscope 2026;136(4):1858–65.
28. Benshetrit G, McAdoo S, Kuchai R, et al. Systemic Immunosuppression to Reduce Surgical Intervention in ANCA-Negative Subglottic Stenosis. Laryngoscope 2026;136(7):3103–10.
29. Eller RL, Livingston 3rd WJ, Morgan CE, et al. Expandable tracheal stenting for benign disease: worth the complications? Ann Otol Rhinol Laryngol 2006;115(4):247–52.
30. Nouraei SA, Nouraei SM, Sandison A, et al. The prefabricated sternohyoid myocartilagenous flap: a reconstructive option for treating recalcitrant adult laryngotracheal stenosis. Laryngoscope 2008;118(4):687–91.
Declaration of competing interests: None declared.
















