Since the beginning of our specialty, generations of patients and surgeons have faced the challenging clinical problem of recurrent respiratory papillomatosis (RRP). Driven by a persistent and chronic infection with low-risk human papillomavirus (HPV) types 6 or 11, it is characterised by recurrent papillomas of the larynx or trachea that recur repeatedly after surgical excision. Finally, after decades of basic scientific discoveries, biotechnological advancements and clinical translational trials, there is a new hope for the treatment of RRP.
Until recently, treatment relied almost entirely on repeated surgical removal of the papilloma's using microdebriders, lasers or sharp instrumentation, which never addresses the underlying chronic infection. As a result, the disease often recurs and most patients require many procedures, sometimes tens or even hundreds of surgeries over their lifetime.
The cumulative impact of repeated surgery is significant. Each procedure carries risks of laryngeal injury – anterior commissure web formation, glottic scarring or decreased vocal cord pliability, and glottic stenosis. Research has shown that higher lifetime surgical counts correlate with worse structural outcomes, through the iatrogenic injury from surgery itself. Even when overt scarring is avoided, the repeated exposure to general anaesthesia, frequent operating-room visits, voice rest and recovery periods take a substantial toll on quality of life, work productivity and emotional wellbeing. Voice-related outcomes often worsen over time due to cumulative damage, even after technically successful debulking.
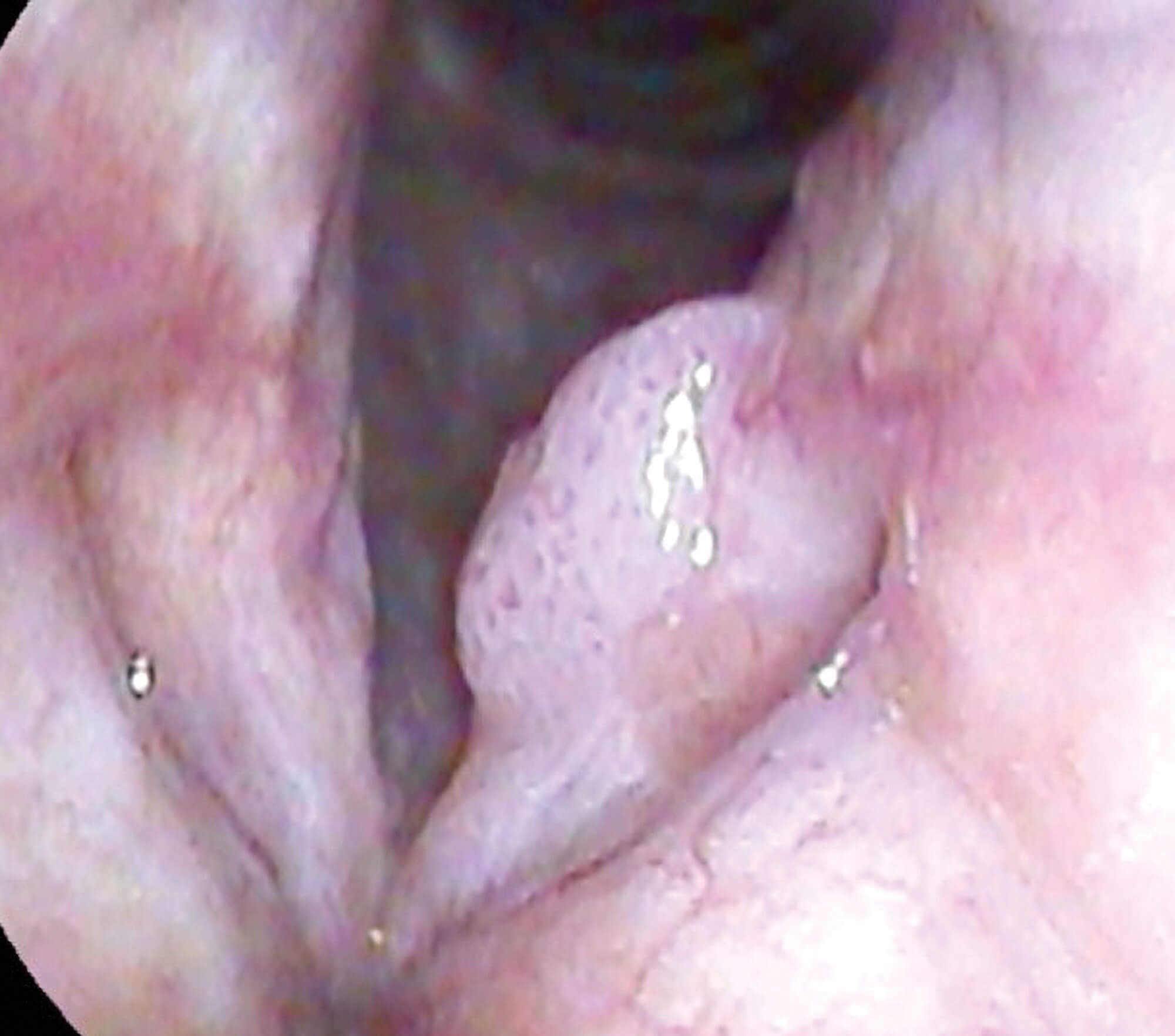
Pre Papzimeos.
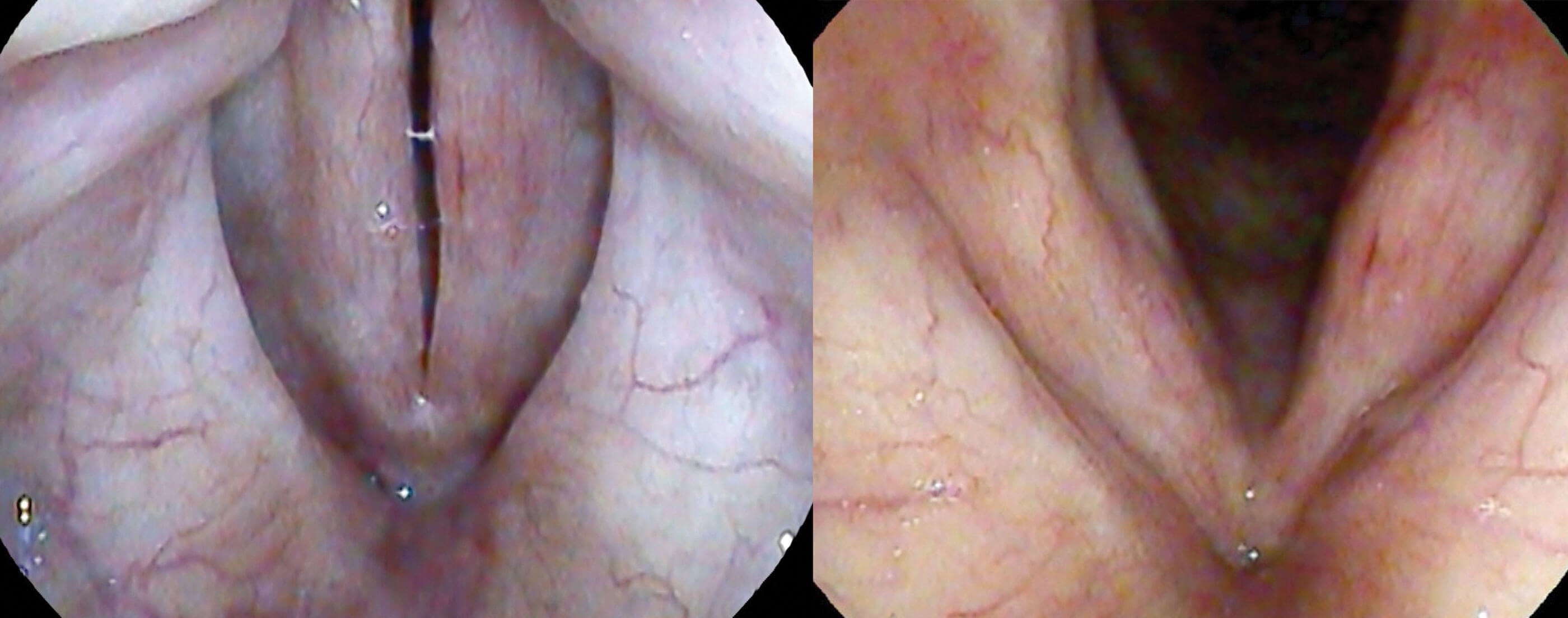
Post Papzimeos.
The recent FDA approval of Papzimeos (zopapogene imadenovec-drba) changes this landscape. Approved by the FDA in August 2025, Papzimeos is the first HPV-specific immunotherapy indicated for adults with RRP. It is a replication-incompetent gorilla adenoviral vector that delivers genes encoding fused proteins from HPV-6 and HPV-11. Administered as four subcutaneous injections over 12 weeks (week zero, two, six and 12), in conjunction with an initial surgical debulking, Papzimeos stimulates a targeted CD8+ and CD4+ T-cell response against HPV-infected cells. Unlike surgery or existing adjuvants, it aims to address the chronic viral infection directly, offering the potential for longer-term disease control after a defined treatment course.
"Papzimeos offers a genuine opportunity to alter the natural history of this disease and meaningfully improve patient quality of life"
The pivotal data supporting its approval comes from a single-arm phase 1/2 trial (NCT04724980) that enrolled adults with aggressive RRP who had required at least three surgical interventions in the prior 12 months. In the 35-patient cohort treated at the recommended dose (5 ×10¹¹ particle units), 51% achieved a complete response – defined as no need for any clinically indicated surgical intervention during the 12 months following treatment start (95% CI 34–69%). The safety profile was favourable: most adverse events were mild to moderate (grade 1–2), dominated by expected injection-site reactions, fatigue, chills and fever. No treatment-related serious adverse events or dose-limiting toxicities occurred. Even more encouraging, many of these responses have proven durable, with some trial participants now over three years without a need for repeat surgery.
Additional analyses from the same treatment cohort showed clear functional benefits. Greater reductions in the Derkay anatomic score (a standard measure of papilloma burden) were strongly associated with fewer subsequent procedures and larger improvements in Voice Handicap Index-10 (VHI-10) scores. Patients who reached complete response frequently moved from moderate-to-severe voice handicap into the mild or minimal range, demonstrating that effective disease control translates into meaningful preservation or recovery of voice function.
In their approval notice, the FDA specifically referenced the biomarker work from the trial that provided insight into response patterns. Patients with complete responses tended to have lower baseline HPV gene expression in their papillomas, stronger interferon pathway activation, higher levels of T-cell-attracting chemokines (CXCL9/CXCL10) and greater intralesional T-cell infiltration induced by the immunotherapy. Non-responders more often showed higher HPV expression, elevated CXCL8 and a neutrophil-dominated microenvironment with fewer T cells. Even though the trial was not randomised or placebo-controlled, these biologic correlates of disease response provided very strong evidence that inducing the T-cell response was in fact the mechanism for the clinical improvement seen. Furthermore, these patterns suggest future possibilities for patient selection or mechanisms of immune escape to target in the future.
In early 2026, the Recurrent Respiratory Papillomatosis Foundation (RRPF) and key opinion leaders in the field published an updated treatment algorithm that positions HPV-specific immunotherapy as a preferred first-line medical option for adults with RRP. After initial diagnosis and confirmation of HPV genotyping, Papzimeos should be considered first-line treatment due to its finite dosing schedule, favourable tolerability and potential for durable remission. The RRPF algorithm stresses shared decision-making and helping patients weigh the cumulative risks of repeated surgery against the benefits of immune-based therapy.
From a practical standpoint, Papzimeos administration should fit smoothly into otolaryngology workflows. The four-dose subcutaneous regimen can be given during office visits, typically coordinated with an initial debulking procedure in the operating room and office-based laser as needed during the 12-week dosing window. Follow-up continues with standard endoscopic surveillance, with the hope of sustained disease remission or reduced disease burden. For complete responders, this can mean years without surgery, substantially reducing laryngeal trauma and anaesthesia exposure. Partial responders still benefit from fewer procedures and less cumulative damage.
Several caveats warrant discussion. Approximately 49% of patients do not achieve complete response; in these cases, systemic bevacizumab is recommended as a second-line option for those wishing to avoid a return to surgery. Data on long-term durability is still lacking, and the current indication is limited to adults. Cost, access and insurance coverage will inevitably influence uptake, particularly in resource-constrained settings. Nevertheless, the safety and efficacy profile of Papzimeos supports broad integration into clinical practice.
The landmark approval of Papzimeos marks the first time otolaryngologists can offer adult RRP patients a therapy that targets the underlying viral infection rather than merely debulking its consequences. By inducing HPV-specific cellular immunity, this novel adenoviral vector immunotherapy has demonstrated the capacity to deliver complete, durable responses in over half of treated patients while simultaneously improving voice outcomes and reducing surgical burden. The RRPF management algorithm provides a framework for incorporating Papzimeos into contemporary care pathways and encourages providers to conceptualise RRP as a treatable chronic infection rather than a surgical problem.
For surgeons who have long managed the relentless cycle of RRP surgery, Papzimeos offers a genuine opportunity to alter the natural history of this disease and meaningfully improve patient quality of life. Ongoing registries and real-world experience will further refine optimal sequencing, combination strategies and long-term outcomes, but the foundational shift from surgery to disease-modifying immunotherapy has already begun.
Further reading
1. Best SR, Friedman AD, Rosen CA, et al. Recurrent Respiratory Papillomatosis Foundation Position Statement on the Management of Adults With RRP. Laryngoscope 2026 [ePub ahead of print].
2. So RJ, Hillel AT, Motz KM, et al. Factors Associated with Iatrogenic Laryngeal Injury in Recurrent Respiratory Papillomatosis. Otolaryngol Head Neck Surg 2024;170(4):1091–8.
3. Kaskas A, Valdez J, Napier S, et al. Disease Control and Voice Outcomes Following Treatment With PRGN-2012 in Adults With Recurrent Respiratory Papillomatosis. J Voice 2025;S0892–1997(25)00163–8.
4. Norberg SM, Valdez J, Napier S, et al. PRGN-2012 gene therapy in adults with recurrent respiratory papillomatosis: a pivotal phase 1/2 clinical trial. Lancet Respir Med 2025;13(4):318–26.
5. Norberg SM, Bai K, Sievers C, et al. The tumor microenvironment state associates with response to HPV therapeutic vaccination in patients with respiratory papillomatosis. Sci Transl Med 2023;15(719):eadj0740.
Declaration of competing interests: SB is a consultant for Inovio Pharmaceuticals and Precigen Pharmaceuticals.







