Some patients would like to alter the appearance of their nose without surgery or make further subtle changes after a rhinoplasty. Lydia Badia explains how this can be done, thanks to the advent of injectable fillers.
This medical procedure in which injectable fillers are used to improve the aesthetics of the nose is becoming a very popular option for patients who aren’t ready to have a surgical rhinoplasty or for those who have had a rhinoplasty but still have concerns. The author also uses a biostimulatory filler to improve the collagen of the soft tissues prior to surgical reconstruction.
The procedure is not intended to replace a surgical procedure. The technique has inherent limitations; it cannot change the structure of bone or cartilage, and it can correct only with an increase. Mullen and Hunter, in their two-part article published in the Aesthetics Journal, gave an excellent overview of the non-surgical rhinoplasty and the nasal anatomy relevant to the procedure and its inherent risks [1].
“The most important anatomical consideration is the vascular network and the potential risk of intravascular injections”
Injection technique
The author uses a combination of a blunt 25G pix’L cannula for supraperiostal-supraperichondrial injections and a sharp 29G needle for intradermal injections. Injection into areas with signs of infections and acne should be avoided. The treatment area should be cleaned with 70% alcohol and aseptic conditions maintained during the injection. The product used is a hyaluronic acid (HA) filler or polycaprolactone with lidocaine. The most important anatomical consideration is the vascular network and the potential risk of intravascular injections.
Serious complications, including blindness and facial skin necrosis, have been reported after HA injection in the nasal and periorbital region. To minimise this risk, the author uses blunt cannulas (25G or wider) in the subcutis and sharp needles only intradermally. Constant movement of the cannula/needle and injection of minimal volumes reduce the risk further. Injecting small amounts slowly also reduces the risk of pressure-related vascular compromise. In the nasal tip, the benefit of a superficial (intradermal/hypodermal) injection with a thin needle is the achievement of a better tip definition.
Deep injection (directly on the cartilages) usually requires larger volumes of product and may widen the lower lateral cartilages. Although it is important to minimise the risk of complications, it is equally important to be prepared to manage complications that may arise. Dr Patrick Treacy published an overview of the management for dermal filler-induced facial artery occlusion [2].

Indications
1. Dorsal hump
A low radix, dorsal hump and inadequate tip projection is one of the commonest complaints in patients seeking rhinoplasty. A better balance with an illusion of straightness can be achieved by injecting at the radix, below the hump and the tip.
A HA filler is injected at the radix and bony dorsum and massaged into a fan shape, narrowing caudally towards the dorsal hump. The purpose of this point is to raise the level of the radix to the upper lash line. The second area of injection is caudal to the hump prominence. The filler may be gently massaged to lead gently into the lower third of the nose. Finally, a small volume of HA is injected at the two light reflection points of the tip. This volume is highly variable, typically 0.05-0.1ml, and depends on the shape of the tip and the response of the soft tissues to the filler injection. These injections help to raise the tip slightly giving a very mild supratip break. Figure 1 shows the profile of a young female patient before and after injection of HA.
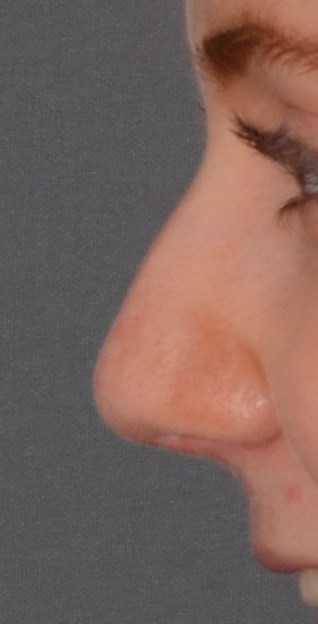
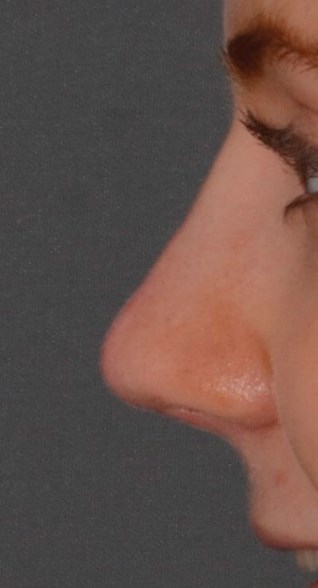
Figure 1. A young female patient before and after injection of HA.
2. Augmentation rhinoplasty
- Saddle nose deformity refers to damage to the cartilaginous middle vault that can leave a deep depression and clear step below the bony upper third at the rhinion. Common causes of saddle nose deformity are trauma, over-aggressive surgery, autoimmune disease and cocaine abuse.
- The Asian population may wish to have higher nasal bridge.
- Post-surgery deformities. Pollybeak deformity or the ‘hooked’ appearance of the nose is seen when the bony dorsum has been reduced, but the mid-third has not been lowered to correspond and gives a classic ‘parrot’s beak’ shape to the lower two-thirds of the nose. Inverted ‘V’ deformity is also a postoperative appearance and is due to the detachment of the upper lateral cartilages from the nasal bones. This leads to the upside down ‘V’ deformity at the junction of the upper and middle third of the nose.
Figure 2 shows the profile of a lady with a saddle nose before and immediately after treatment with HA filler.


Figure 2. A lady with a saddle nose before and immediately after treatment with HA filler.
Figure 3 is of a lady with several post-rhinoplasty deformities who was seeking revision surgery; she had HA fillers in the interim.


Figure 3. A lady with several post-rhinoplasty deformities who was
seeking revision surgery; she had HA fillers in the interim.
3. Post-traumatic deviations/depressions
The author uses a biostimulatory filler to improve the collagen of the soft tissues prior to surgical reconstruction in patients with a damaged soft tissue envelope. The collagen stimulatory effect has recently been confirmed in humans on skin biopsies from treated subjects.
“Injecting small amounts slowly reduces the risk of pressure-related vascular compromise”
The injection technique is with a 25G cannula. Local anaesthesia (0.05 ml of xylocaine with 2% adrenaline) is injected in the infratip lobule. The cannula is inserted between the domes of the lower lateral cartilages and passed along the nasal dorsum. We believe subcision is essential prior to the deposit of the biostimulatory filler. It breaks down tight scars and allows for a more evenly distributed product.
Having non-surgical rhinoplasty is a procedure which can give a temporary improvement in the appearance of the nose and it may be an option for patients depending on their circumstances. Having fillers in the nose is not a contraindication to having surgery at a later date.
References
1. Mullen G, Hunter B. Non-surgical Rhinoplasty. Aesthetics Journal 2016:34-6.
2. Treacy P. Prime Supplement - Jan 6, 2015.
https://www.slideshare.net/ptreacy/
prime-supplement-dr-patrick-treacy
Last accessed May 2019.
Declaration of Competing Interests: None declared.



