We, at ENT & Audiology News, have just learned of the death of Professor Heinz Stammberger on 9 December. Within the global ENT community, there can be few people whose names are as well-known as his, and his loss will be keenly felt around the world. A private funeral took place on 15 December. We extend our sincere condolences to his family and friends.
Here we have gathered a selection of tributes from some of his close friends and colleagues. We will continue to add to these as more come in.

Please click here to view this tribute on the European Rhinologic Society website.
“I am telling you Heinz, the name Stammberger means a lot more to people than sinus surgery”
“Muaaz, I think you are imagining stuff.”
I cannot recall how many times I had the above exchange with Heinz, I think his retort reflects how he truly saw himself. But everybody else saw him differently. As we grieve his loss and as I exchange messages and conversations with colleagues around the world, I am more convinced than ever that Heinz’s legacy means a lot more to the global ENT community than his innovations in endoscopic sinus surgery.
Firstly and most of all, beyond his German and Austrian roots, he was a true globalist, he loved all sorts of terrains, people, cultures and religions. He was fascinated by all and felt that our problems, solutions and the way forward are rooted in that global view. He was as committed to teaching surgeons in the far corners of the world as he was to his Austrian and European compatriots.
Secondly, Heinz wanted to do the right thing for only that reason. He also expected others to do the same and could not understand why anybody would not. Although he was very accepting of the different levels of skills and education around the globe and was willing to work with everyone, he did not accept mediocracy when based on mental laziness. He viewed with contempt surgeons who refused to learn and who have a grandiose perception of themselves, especially when that results in patients suffering.
Thirdly, He was truly intrigued by his field. Everything about the sinuses fascinated him; he was amazed by the anatomy, pathophysiology of sinus disease and how surgical treatment can be enhanced by technology. In a way, he retained the little child attitude of curiosity and constant amazement.


Prof Stammberger during a tour of the TSESI building project in Dubai, April 2018.
Lastly, he was a teacher.
I am more determined than ever to preserve his legacy and to make sure that younger ENT surgeons for generations to come will recognise his contributions and his true character. TSESI: Tarabichi Stammberger Ear and Sinus Institute will make sure of that through continuous scholarships, courses and research.
Although Heinz left no offspring, many of our younger colleagues will continue to view him as the father of endoscopic sinus surgery.
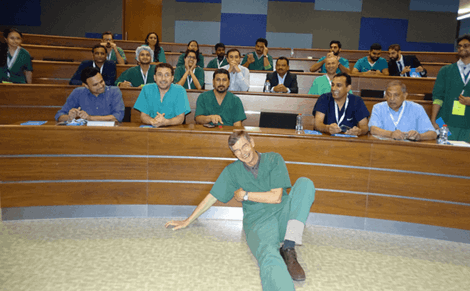
Professor Stammberger resting after a busy day teaching at the October 2018 TSESI Course.
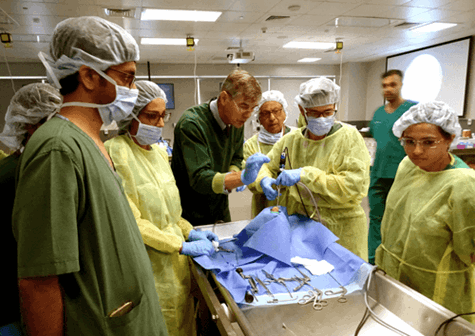
Professor Stammberger engaging trainees at the October 2018 TSESI Course.

All happy after a very intensive course at the October 2018 TSESI Course.

Group photo with Professor Stammberger at the October 2018 TSESI Course.
Muaaz Tarabichi, Head of ENT Department, American Hospital Dubai, UAE.
Heniz Stammberger was involved in sponsorship of scholarships for young residents and left an impression on many of them. On the following link, you will find videos from those students recounting their memories of Professor Stammberger.
http://www.tsesi.org/in-memory-of-heinz-stammberger/
As I write, I am still stunned and deeply saddened by the news of the loss of Heinz Stammberger. He has been a core figure in rhinology from my very first days in ENT and it is impossible to contemplate holding a meeting without his wry smile and words of immense wisdom. Without his contribution to rhinology, I am quite sure that we would not have the thriving specialty that we have today.
As an SHO I was captivated by endoscopic sinus surgery, still in its relative infancy. I learnt of the Stammberger technique, bought the textbook, and sat in awe at his lectures. Heinz lived in the realms of the rhinology gods; I eagerly joined the audience as we hung on his every word and once even joined a queue of juniors at a meeting to take a selfie with his cardboard cut-out (he famously refused all requests for photos with the ‘real deal’). His allure never faded, as rhinologists young and old were drawn by his passion, charm, experience and never-ending patience for the endless questions that came from the audience.
"He was an incredibly warm, intelligent, thoughtful and humble man."
As I progressed in my career I was initially equally terrified and delighted to be asked to join Heinz on panels, and in teaching together on FESS courses. After every lecture I would eagerly look to Heinz for his approval and, although I am absolutely sure that he had heard everything a million times before, he was always supportive and encouraging. I am grateful and immensely privileged that I had the opportunity to work with him, learn from him and get to know him. He was an incredibly warm, intelligent, thoughtful and humble man. He was extremely generous with his time and friendship, and his loss will be keenly felt around the world. My thoughts are with his wife, Doloris, and those closest to him.
As I operated today, I smiled and had a moment of quite reflection as I asked for the Stammberger punch. He will continue to inspire generations of rhinologists for many years to come, and will certainly never be forgotten.
Claire Hopkins, Consultant ENT Surgeon, London, UK.
Rest in eternal peace, Professor Heinz Stammberger. Eulogies and condolences are flowing. I am not even sure where to begin. He was a revolutionary; he popularised his teacher, Prof Messerklinger's, concepts of 'less is better' in sinus surgery. He hence became a ‘Custodian’ of functional endoscopic sinus surgery (FESS) for over 30 years.
He was, without doubt, one of the most accomplished, talented, revered, and worshipped stalwarts in the world of rhinology. So focused he was in the promotion and practice of this religion called endoscopic sinus surgery, that every course/workshop he taught in was a stupendous success, every lecture-class, a masterclass and every surgery, life-changing. The charm and magnetism he displayed with his surgical skills are indeed unparalleled and inimitable. I recall his favourite ‘to whet your appetite’ exercise on endoscopic ligation of the sphenopalatine artery and the crowd would be spellbound, following with a thunderous applause...and he would cheekily ask, "Oh, so you want me to stop here?"
Disease alleviation with minimum invasion was his dictum, I reckon. He was such a firm believer of 'First do no harm' (Hippocratic Oath), that he reprimanded publicly those that ‘MESSed with FESS’. My fond memories with him include my long interview feature with him in what was then ‘ENT News’ in 1998, the ERS/EUFOS/BACO meetings, IFOS congresses, RCS and RSM study days, my guru, Dr Kirtane's, workshops, Middle East Otolaryngology meetings and TSESI fellowships (thanks to Muaaz Tarabichi), to list a few. He would simply wave at me and just say “ENT News” with a big smile every time we met. Evergreen is the memory of a cruise down the Danube with him and the faculty and delegates of ERS Vienna 1998.
Prof Heinz, I am glad to have lived in your times. Thanks for everything that I have virtually learned from you and your textbooks, lectures and publications. Hey man, what a phenomenal leader you have been!
Sunil Narayan Dutt, Senior Consultant and Clinical Director, Department of Otolaryngology (ENT) & Head-Neck Surgery, Bangalore, India.
Read Sunil’s 1998 interview with Professor Stammberger below.
In 1998, at the ERS and ISIAN meeting in Vienna, Sunil Dutt caught up with Professor Heinz Stammberger to talk about his remarkable career in rhinology. Here, we look back at this wonderful interview.
Congratulations on being elected President of the European Rhinological Society (ERS) and the International Symposium on Infection and Allergy of the Nose (ISIAN). You have already contributed immensely to the field of rhinology. What more do you think you can offer in your new role?
I see it as one of my tasks to help generate something like a 'corporate identity' for members of the European Rhinologic Society. This will include establishing quarterly newsletters with information on past and upcoming international, national and local meetings, news on awards and other personal achievements of rhinologists etc. This will not be in competition with any other publication, but will rather augment the scientific information with some more academic, social and society news. I would like to induce a 'community feeling' amongst European rhinologists and their cooperation with rhinologists worldwide.
What are the issues in rhinology that deserve immediate attention?
The ERS & ISIAN Meeting in Vienna has impressively demonstrated that basic and clinical research are very strong in our specialty, with evidence of high levels of activity in all fields of rhinology. It is impressive to see the change, for instance, in our understanding of nasal polyposis. Here research on eosinophils, mediators and immunologic processes is gradually translating into modification of our surgical and medical therapy. One of the many problems is to prove (in the sense of evidenced-based medicine) that one kind of surgery is 'better' or more effective than another. Most of all, we lack proof as to whether surgery has a role at all in the various inflammatory processes of the nose and sinuses. It will be one of the challenges of the future to answer these questions.
Why do you think endoscopic sinus surgery has been taken up so widely?
There is no easy answer to this question. Endoscopy in the true sense of the word has shed light on the hidden clefts and poorly visible recesses of the sinuses. It has thus enhanced our understanding of the pathophysiology of sinonasal disease. We appreciate that the sinuses we have focused on previously - frontal and maxillary - are not usually the site of origin of disease. Endoscopic diagnosis has coincided with important developments in CT imaging, augmenting findings of ostiomeatal complex disease. Therapy - not necessarily surgical - is now directed to these areas, clearly improving the situations. For those having been brought up with inferior meatal fenestration and radical approaches to the maxillary sinus as a first choice of treatment, the change of concept (and the results!) have been impressive.
(R-L): Sunil Dutt and Professor Heinz Stammberger at the conference in Vienna.
Unfortunately the concept of FESS is still not fully understood in many places. The full concept includes a diagnostic approach and an effort to avoid surgery or at least unnecessary radical surgery - as opposed to using the endoscope as an optical device with which to perform the radical approaches of the past.
One might add the fascinating possibilities of the endoscope in postoperative care. In fact, we can see the changes of the mucosa for better or worse, and recognise diseases in early stages, when medical therapy can still be successfully employed. Of course there is the fascination of extended applications - like detection and closure of CSF-leaks, correction of meningoencephaloceles, orbital and optic nerve decompression, mucocele surgery and so on.
We should not forget that inflammatory diseases of the nose are diseases that should primarily be treated medically and only if such therapy fails should surgery be considered. The dark side of the endoscopic surgery fascination in my eyes is that it is used with too little critique and far too frequently.
What, according to you, is a correct protocol for a training programme in FESS?
There is no single answer to cover all the problems of a training programme for FESS. Of course this should include:
- Watching diagnostic and surgical procedures for many months before picking up an endoscope oneself.
- A long period of familiarisation i.e. practising diagnostic endoscopy and understanding differences in the handling of a 0, 30, 45, 70 degree telescope.
- The next step should be undertaking postoperative care under endoscopic guidance.
- The last step is surgery in selected cases.
For this last step, we favour Prof Arnold Maran's recommendation of a 'traffic-light' approach:
Green for the anterior ethmoid up to the basal lamella of the middle turbinate; yellow posterior ethmoid and sphenoid sinus and red (the most difficult area) the frontal recess and the frontal sinus region.
The latter should only be approached with utmost care and after having achieved significant experience in the technique. Cadaveric training is the best opportunity to get acquainted with the variable anatomy. The residents at our department are not introduced to endoscopic surgery until the end of their fourth year of training. As in all surgical fields, the dexterity of surgeons can be improved by teaching and training, whereas a teacher cannot instill talent.
What are your general thoughts on FESS in children?
I would like to refer you to a publication by Valerie J Lund, HJ Nejens, PAR Clement, R Lusk and myself published in the International Journal of Paediatric Otorhinolaryngology, 1995, (32), (Suppl.) S.21-S.35, following a symposium on: 'The Treatment of Chronic Rhinosinusitis in Children: A Controversial Issue'. It was generally felt at this meeting that there is significantly less need for surgery for sinonasal conditions in children compared with adults. There are good indications, such as certain complications of acute sinusitis, antrochoanal polyps and in cystic fibrosis but these require surgeons with a very high level of experience.
Professor Heinz Stammberger.
Do you believe that powered dissection with microdebriders and shavers is essential, or is it just glamorous to have these instruments as part of one's armamentrarium?
Microdebriders/shavers help a lot in special situations. Personally, I like to use them for diffuse polyposis, especially in revision surgery. There is however some disadvantage in using these instruments: the tactile sensation is decreased and shavers are not a substitute for meticulous technique. Personally I do not like using the curved blades, especially in the frontal recess where I have seen significant damage being caused. At meetings and conferences one is starting to hear reports of disastrous events from their use such as intracranial and orbital entry. As tissue is aspirated and cut as long as 'power is on', these incidents result in significantly greater damage than with conventional instrumentation. We consider it mandatory that shavers should only be used with 'tissue traps' so that all tissue removed can be collected and sent for pathologic examination.
What do you think have been the most noteworthy recent advances in rhinology in general and FESS in particular?
There is no single answer to this question. Personally, I am fascinated by advances in smell research, as highlighted in Vienna by Dr Simmen's panel, the immunological advances in allergic and non-allergic rhinosinusitis and, of course, nasal polyps. In FESS, clearly the extended applications are a true challenge for the experienced surgeon. Intraoperative image-guided computer-assisted surgery is another fascinating field, although the true value in routine procedures has yet to be determined.
Do you think advances in the medial treatment of rhinosinusitis might make surgery (and surgeons!) redundant?
This might happen, though not within the next five years. Certainly diffuse nasal polyposis will turn out to be primarily a medical disease. As more inflammatory genes are identified and perhaps a gene-based therapy modality becomes available, surgery will become less important. However, many patients will continue to present with either complications of sinusitis or with advanced polyps at their first visit, so surgery will continue, although to a lesser extent. For the time being, a combined approach, i.e. medical and surgical, is the therapy of choice.
Finally, what have been the highs and lows of your career so far?
This is a very personal question. Regarding the highs, the presidency of the ERS & ISIAN meeting in Vienna was the latest in a series of extremely gratifying experiences. These started in 1975 with the good luck of working in the ENT department at Graz to work with Prof Messerklinger. The time was just ripe for an endoscopic approach to the nose and I have had the unique chance to help spread the FESS philosophy around the world. The recognition that I have received over the years has made me proud and humble at the same time. I also consider myself extremely fortunate to have had the privilege of meeting so many excellent researchers, clinicians and surgeons over the years and, furthermore, to have made many true and close friends in this community.
As for the lows, there have been few. The most significant though was when I applied for the chair of the late Professor Spoendlin of the ENT-department at Innsbruck University in 1992. It was not the fact that I did not make it which hurt (I do not have a pronounced ego in this regard), but rather the blatant political moves of some of my Austrian colleagues, orchestrating a smear campaign by which they tried to discredit me politically. I have survived though and thoroughly enjoy my work in the field of rhinology. I am happy to head the department of general ENT at Graz University Medical School where I am also engaged in skull base and oncologic head and neck surgery.
Hesham Negm spent many years in the fond company of his good friend, Heinz Stammberger. Here, he shares some of his fondest memories with a selection of wonderful photos including pictures from Cairo University ORL in 2014, a visit to the Hatshepsut temple, The Egyptian ORL Congress in 2008, Hesham's house, and many more...