Surgical training is constantly developing to improve ENT surgeons’ technical and non-technical skills. In this article, Joshua Whittaker, an ENT Registrar and ENT Simulation Fellow at University Hospitals Birmingham, describes the rise of simulation training.
Simulation is the recreation of real-world situations or processes in a controlled environment. Simulation-based education (SBE) is a crucial element of modern medical education across the world, in all specialities and at all stages of training [1].
SBE can provide trainees with a controlled, predictable, and unpressurised learning experience which can be specifically tailored to their development needs. The available time for clinical experience during training has been impacted in sequential generations by the European Working Time Directive, changes to junior doctor contracts and, more recently, the coronavirus pandemic with associated cancellations of elective services. Whether intentional or not, the subsequent pressures to reduce waiting times has demanded greater focus on service provision, sometimes to the detriment of training time. This means the trainees of today have less focused clinical training time to develop their ability than ever before. SBE gives an opportunity for training programmes to supplement clinical training by replicating training experiences away from the clinical environment.
From a patient and healthcare system perspective, SBE allows greater protection of patient safety. Greater ethical scrutiny has been placed on the concept of training on patients, particularly in surgical fields [2]. The adage of ‘see one, do one, teach one’ is outdated and the era of learning through complications is over. Although training with real patient exposure is a vital part of becoming a competent healthcare professional, SBE can provide initial credentialing that trainees are safe to move on to patients without causing harm. SBE also offers methods to practise and maintain less commonly encountered but vitally important skills (High acuity, Low opportunity; HALO).
SBE can be loosely divided into those focused on technical and non-technical skills. Of course, seeing these as mutually exclusive experiences (particularly in surgical specialities) would be naïve: it would be impossible to develop high-level technical skills without parallel non-technical skills. However, the pedagogical processes used to maximise learning in each can be quite different.
Non-technical skills training in SBE
Non-technical skills (NTS) refer to the metacognitive and interpersonal skills required for healthcare professionals to effectively negotiate the complexities of modern healthcare systems, their patients, and other professionals. The non-technical skills for surgeons (NOTSS) behaviour marker system is the most commonly cited description of these in surgical practice [3]. This recognises skills such as communication and teamworking, leadership, decision making and situational awareness.
High-fidelity (highly realistic) SBE is now well embedded in undergraduate and early postgraduate training. This includes the use of simulated patients (specifically trained role-players) and advanced manikins. In fact, most surgical trainees starting a training programme in the UK today will not have experienced training without high-fidelity SBE, making them extremely literate in how to effectively extract learning from this experience. Debriefing, the process of evaluating and analysing simulation performance is the focus of this learning experience. It does not focus on whether the learner’s actions were correct or incorrect, but on the learner’s feelings and understanding as they approached the situation. This framing of the situation affects how clinicians’ access and use their knowledge, technical and non-technical skills. Understanding this is crucial to alter the future reaction to similar situations and, thus, the subsequent actions taken (hopefully for the benefit of patient care) [4].
In-situ simulation is an extension of this, where the simulated patient or manikin is brought into the real clinical environment, sometimes without prior notice to the team working there. This enables teams to not only have deliberate practice of their NTS, but to identify latent system errors and human factors in their everyday clinical environment before they impact on real patients. In-situ simulation tends to be more focused on team performance than the individual, and therefore has a key role in enhancing the performance of the entire surgical team.
Advances in virtual reality (VR) technology, have led to rapidly-progressing immersive environments that can be delivered with little more than a VR headset and the correct software. These are starting to be combined with artificial intelligence programmes which can enable virtual avatars to react and converse with the learner in a meaningful and realistic manner. There is limited application of this specifically in ENT but the rapid growth of the field no doubt means this is not far from realisation.
SEE ALSO
SBE for NTS is growing in popularity in surgery and can be delivered to replicate emergency department, ward, clinic, and operating theatre environments. These will likely become a normal part of surgical training and surgical team skill maintenance. As such, it is vital that surgical trainers and trainees develop an understanding of how to use these tools to effectively learn.
Technical skills training in SBE
Technical skills refer to the practical or procedural abilities of clinicians, such as surgical skills. I have already highlighted how training hours for deliberate practice is limited in modern healthcare. Very few trainees in any field will gain enough experience within their clinical training to reach mastery, but SBE can provide additional training hours towards this goal.
Simulation in surgical skills is well established. For hundreds of years, dissection of animal and human cadaveric tissue has been used to learn anatomy and develop operating dexterity. In ENT, cadaveric surgical simulation courses are common for temporal bone dissection, endoscopic sinus surgery, head and neck surgery, nasal surgery, facial plastics and laryngological procedures. However, non-bleeding cadavers have limitations in realism, and are an extremely limited and expensive resource, not to mention the complexity involved in delivering training within the remits of the Human Tissue Act.
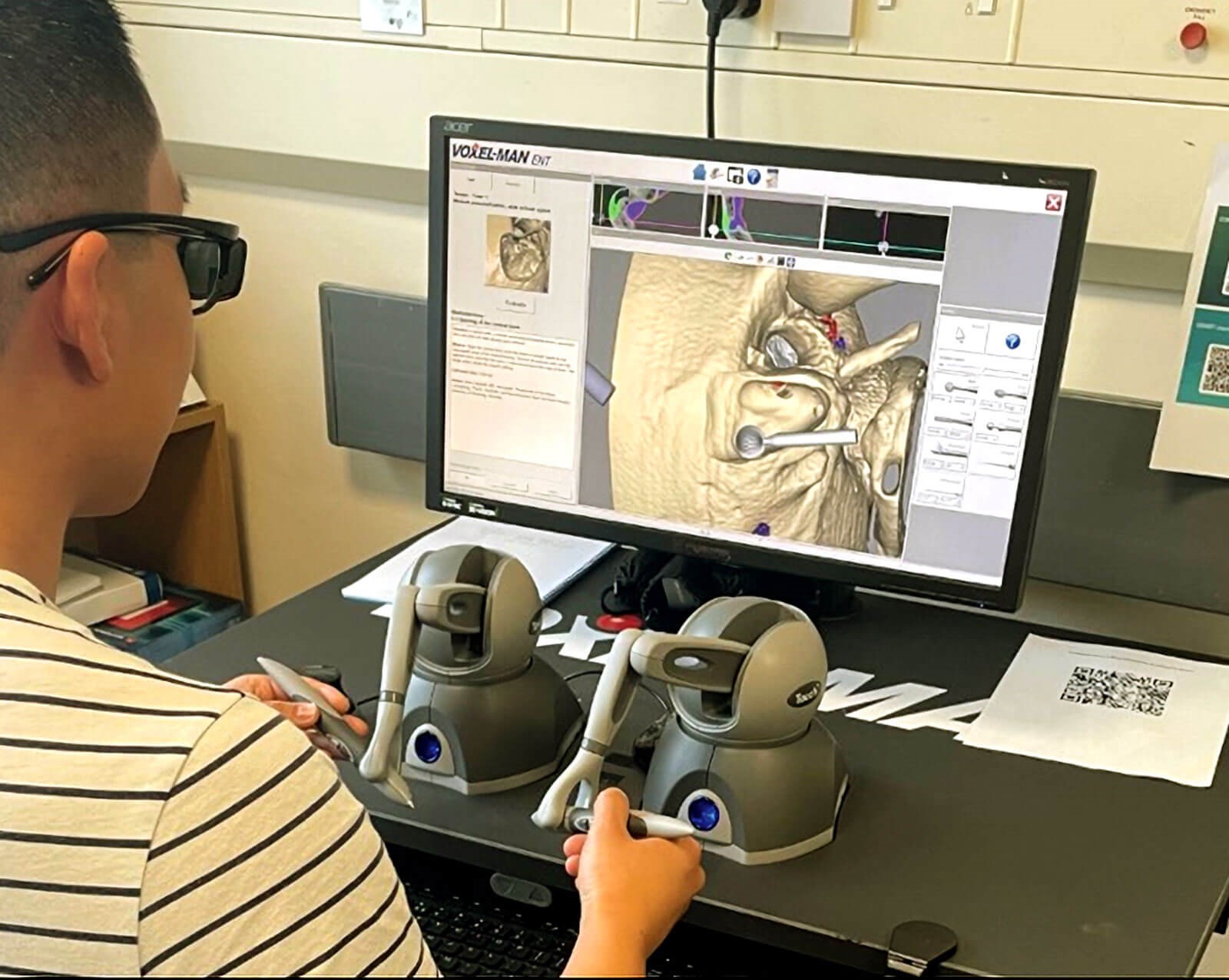
Figure 1. Digital temporal bone dissection simulator.
This console is produced by VOXEL-MAN but others are available.
In recent years, technological advances have enabled the creation of non-cadaveric surgical simulators of varied complexity for various procedures. A 2016 systematic review identified 54 validated simulators in ENT training. The most common were ear and temporal bone stimulators, followed by those for laryngology and endoscopic sinus surgery [5]. Amongst these are VR and digital simulation consoles which are operated on with haptic feedback instruments using three-dimensional (3D) glasses (Figure 1).
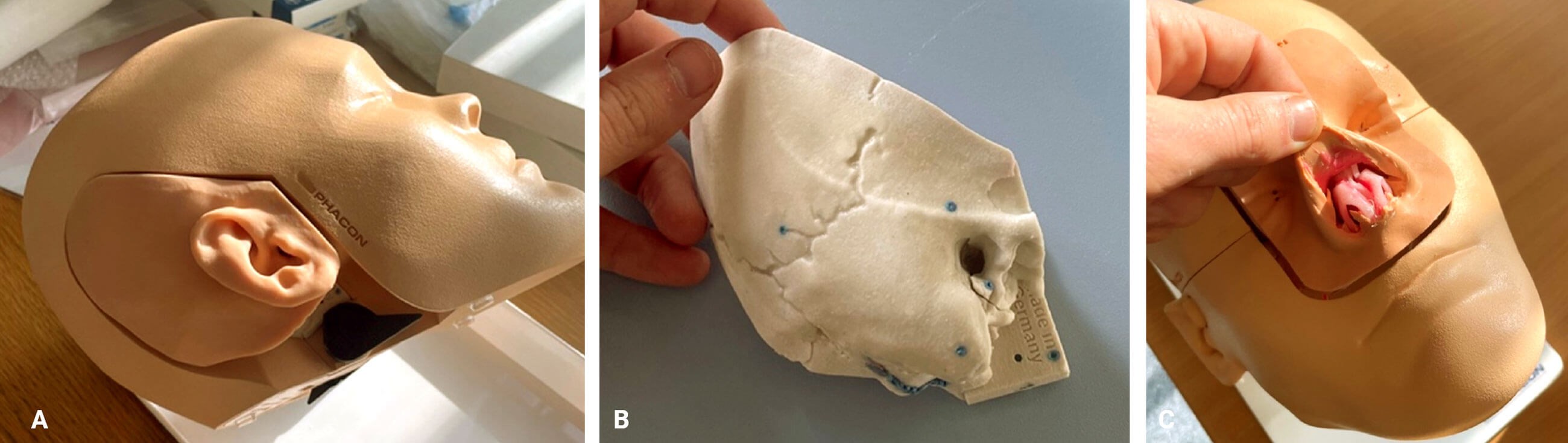
Figure 2. Temporal bone models – with soft tissue (A) and without (B). (C) Nasal surgery models capable of delivering training in septorhinoplasty (closed and open), functional endoscopic sinus surgery, sphenopalatine artery ligation and endoscopic dacrocystorhinostomy (DCR). These models are produced by Phacon but other validated models are available.
Also, in use are ‘dry’ models: 3D-printed models of regional anatomy which can be operated on with genuine surgical instruments (Figure 2). Despite their relative complexity of production and large initial capital investment, these resources represent a significantly more cost-effective method to deliver repetitive deliberate practice than cadavers. They give trainees a greater scope to ‘stop and reset’ the simulators to repeat individual steps multiple times in quick succession.
Delivering the simulation-based education of tomorrow
The delivery of these resources has enormous regional variation in the UK. There is no current national curriculum for SBE in ENT. A growing body of evidence is starting to identify how these different resources will complement each other and the benefits they can have for training. However, there is still a paucity of high-quality evidence for the educational benefit. This is common across many specialities. The ultimate aim of SBE is to create more skilled clinicians delivering better patient outcomes. This is very difficult to conclusively demonstrate without confounding other factors in the healthcare system. We therefore must assess effectiveness using proxies such as objective changes in skill or knowledge, or by collecting meaningful qualitative data. Consequently, this means we need trainers and trainees that are literate in educational theory and educational research principles.
Ultimately, the future training of ENT needs to use SBE to supplement and enhance traditional clinical experience. This needs to be delivered in a deliberate and coordinated manner to introduce, develop and maintain surgical and non-technical skills in our workforce for the benefit of our colleagues, employers and, above all, patients. ENT is currently ahead of the curve in this regard and has an opportunity to be the example to which all surgical training could aspire.
References
1. Motola I, Devine LA, Chung HS, et al. Simulation in healthcare education: A best evidence practical guide. AMEE Guide No. 82. Med Teach 2013;35(10):e1511-30.
2. De Montbrun SL, Macrae H. Simulation in Surgical Education. Clin Colon Rectal Surg 2012;25(3):156‑65.
3. Yule S, Flin R, Paterson-Brown S, et al. Development of a rating system for surgeons’ non-technical skills. Med Educ 2006;40(11):1098‑104.
4. Rudolph JW, Simon R, Rivard P, et al. Debriefing with Good Judgment: Combining Rigorous Feedback with Genuine Inquiry. Anesthesiol Clin 2007;25(2):361-76.
5. Musbahi O, Aydin A, Al Omran Y, et al. Current Status of Simulation in Otolaryngology: A Systematic Review. J Surg Educ 2017;74(2):203‑15.







