A minimally invasive temporal craniotomy using an exoscope offers improved visualisation, ergonomics and recovery for middle fossa dural CSF leak repair.
Cerebrospinal fluid (CSF) leak through a dural defect, regardless of the cause, typically requires surgical repair. Depending on the underlying cause, additional strategies to decrease intracranial pressure can also be considered [1]. Lateral skull base CSF leaks can cause headache, hearing loss and tinnitus, and risks meningitis and encephalocele formation.
The choice of surgical approach for repair of lateral skull base CSF leaks is influenced by the site of the defect, surgical preference/experience and certain patient-related factors. While posterior or lateral defects may be addressed via a transmastoid approach, temporal craniotomy is usually required to access anterior, medial or multiple defects [1]. There are pros and cons for both approaches. Temporal craniotomy is performed by lifting a craniotomy bone flap, which is removed temporarily during the procedure. This gives excellent exposure but requires a larger incision and temporalis muscle dissection. The transmastoid approach offers reduced morbidity and length of stay but can suffer from the usual pitfalls of performing otology surgery with a microscope: narrow field of view with limited exposure of the surgical site, ergonomic constraints and limitations for teaching.
"Lateral skull base CSF leaks can cause headache, hearing loss and tinnitus, and risks meningitis and encephalocele formation"
As exoscope technology has advanced, particularly with respect to image resolution and depth perception, their applicability in the field of neurotology is increasing [2]. Exoscopes offer excellent magnification, comfortable ‘heads up’ working position with bimanual operating, high-resolution shared screen, and they can offer an advantageous view angle for dealing with lateral skull base defects.
Technical description
The authors describe middle fossa dura repair via a minimally invasive temporal craniotomy using an exoscope (VITOM® eagle 4K-3D from Karl Storz, Tuttlingen, Germany).
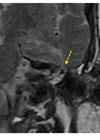
This patient had an iatrogenic dural defect with two previous attempts at reconstruction and was referred to our centre for definitive treatment. The patient had a very small, sclerotic mastoid with prominent sigmoid sinus restricting a transmastoid approach, and the defect was situated medially at the anterior attic (Figure 1).

Figure 1: Computed tomography showing the sclerotic left mastoid (*) and prominent sigmoid on the axial plane (A) and the bony defect and site of CSF leak (arrows) on coronal plane (B).
Following standardised neurotology theatre procedure, a C-shaped post-auricular incision and periosteal flap is made and a small craniotomy is placed at the level of the defect just over the external auditory canal in a staged manner using an otology drill (Figure 2).

Figure 2: Exoscopic view showing the mini craniotomy just over the left external auditory canal (EAC) at approximate size under 15 mm (width) by 8 mm (height) (size 4 mm burr) being created (A), offering adequate access to elevate the middle fossa (MF) (B) and identify the tear and CSF leak source (highlighted with dotted, curved line and dotted arrows) (C); a shaped sheet of Neuro-Patch® was used to reconstruct the defect (D).
With the help of the exoscope and gentle elevation of the middle fossa, without any retraction, the dura defect and source of CSF leak is identified (Figure 2).
The minimally invasive craniotomy gives a great view of the area of interest with the exoscope and adequate access for haemostasis and manoeuvring. With gentle elevation, a sheet of Neuro-Patch® (a synthetic, nonabsorbable microporous patch from B.Braun, Melsungen, Germany, which we have demonstrated in previous publication [3]) is cut to size and placed onto the dural defect in an overlay technique completely covering the defect (Figure 2).
An intraoperative Valsalva manoeuvre is used to ensure adequate sealing of the defect and absence of any persistent CSF leak. A small amount of temporalis muscle with TISSEEL® (a fibrin sealant from Baxter UK, Reading, United Kingdom) is applied to cover the mini craniotomy for additional stability before closure of the periosteal flap and skin in layers. The patient is admitted overnight for routine neurotology observation and discharged the next morning.
"The minimally invasive craniotomy gives a great view of the area of interest with the exoscope and adequate access for haemostasis and manoeuvring"
At a four-week follow-up appointment, the patient had fully recovered, without any indication of residual CSF leak; hearing was also preserved.
Discussion
With an increasing number of patients with spontaneous CSF leak, it is important to optimise repair approaches and techniques in order to improve outcomes and shorten patients’ recovery and stay. The authors present an alternative to open craniotomy and transmastoid approaches for repair of a middle fossa dura defect, using the exoscope to facilitate minimally invasive drilled craniotomy. While the surgical microscope has certain advantages and also allows bimanual access, which is critical for such cases, the exoscope provided better visualisation and allowed us to avoid a traditional middle fossa craniotomy, which incurs additional risks and prolonged hospitalisation.
The use of the exoscope for such cases is an evolving technique and application. In the author’s experience, this approach allowed effective visualisation and repair of the dural defect, superior to that which would have been possible with an operating microscope, given the tight anatomy. The ergonomic design and the shared display of the exoscope gave the surgical first assistant a superior view in a comfortable position, which aided surgical progress and enhanced teaching. Primarily, though, the advantageous visualisation provided by the exoscope allowed us to perform a minimally invasive approach, which shortens and enhances the patients’ recovery. Further use of this device and technique should provide additional evidence.
References
1. Spinos D, Varoutis P, Geropoulos G, et al. Surgical Outcomes Comparison of Spontaneous Middle Cranial Fossa Cerebrospinal Fluid Leaks: Systematic Review and Meta‐analysis. Otolaryngol Head Neck Surg 2025;173(1):27–39.
2. Di Bari M, Colombo G. Exoscope-assisted surgery in otology and neurotology. Curr Opin Otolaryngol Head Neck Surg 2024;32(5):301–5.
3. Wales R, Chakravarty D, Gilmour E, Kontorinis G. The Use of Synthetic, Nonabsorbable Graft for Middle Fossa Repair in Patients With Spontaneous Cerebrospinal Fluid Leak: A Pilot, Prospective Study. Otol Neurotol 2024;45(8):e576–80.
Declaration of competing interests: None declared.