For audiologists and patients alike, the technical challenges of fitting hearing aids for music are well known. Drs Greasley and Crook introduce their research and top tips for improving satisfaction in this important topic.
Hearing aids are often problematic for music perception, with listeners frequently reporting issues such as a lack of clarity, poor sound quality and distortion [1,2]. Music plays a key role in people’s health and wellbeing through functions such as emotional regulation, reduction of negative states (e.g., anxiety, loneliness) and social connectedness, and music is increasingly used in clinical and care settings with older adults to manage conditions such as dementia, Alzheimer’s and Parkinson’s Disease. It is important therefore to address problems that hearing aid users experience with music in order to enable continued musical participation.
Audiologists are rarely taught about programming hearing aids for music during their training and, whilst a small number of audiology clinics and audiologists specialise in music, there is little empirical evidence about the strategies being used [1]. Nearly a decade ago, Chasin and Hockley put forward suggestions based on their clinical practice for managing issues with music listening [3]. This included setting similar WDRC parameters for speech and music, adjusting bandwidth depending on degree of hearing loss, and disabling automatic functions for speech. However, it is not clear whether audiologists have been using such strategies, or whether they lead to improved outcomes.
“We asked audiologists to reflect on any training, the extent and outcomes of discussions about music, and their experiences and confidence in programming hearing aids for music”
As part of the Hearing Aids for Music (HAFM) project (www.musicandhearingaids.org), a collaboration between the University of Leeds and Sheffield Teaching Hospitals NHS Trust investigating how hearing impairment and hearing aids affect music listening, we devised a study to explore the ways in which audiologists address musical needs in clinic [1]. We asked audiologists to reflect on any training, the extent and outcomes of discussions about music, and their experiences and confidence in programming hearing aids for music.
Ninety-nine audiologists completed the survey. They represented a spread of ages (22-71 years), clinical experience (years practising: 49% <10 years, 51% >10 years) and sectors (62% public, 23% private, 10% public and private, 1% charity, 4% unknown), and the majority of their day-to-day practice was reported to be fitting binaural BTE hearing aids. Very few had received formal training on music, though a third (37%) reported some training through conferences, continuing professional development or manufacturer-led workshops.
“Our study is one of the first to map empirically the strategies that audiologists are using to address musical needs in clinic”
A majority (85%) had discussed music with patients, though the frequency of discussions about music varied with some (13%) asking four out of five patients, but half asking one in five patients or fewer. Around 60% reported some confidence in providing advice about music and in fitting hearing aids for music, though 25% were ‘not sure’ and 17% were ‘quite reluctant’ to do so, highlighting a need for greater knowledge and training in this area. Positively, having had some training was associated with confidence in providing advice, confidence in programming hearing aids for music, and in programming hearing aids for a greater number of patients.
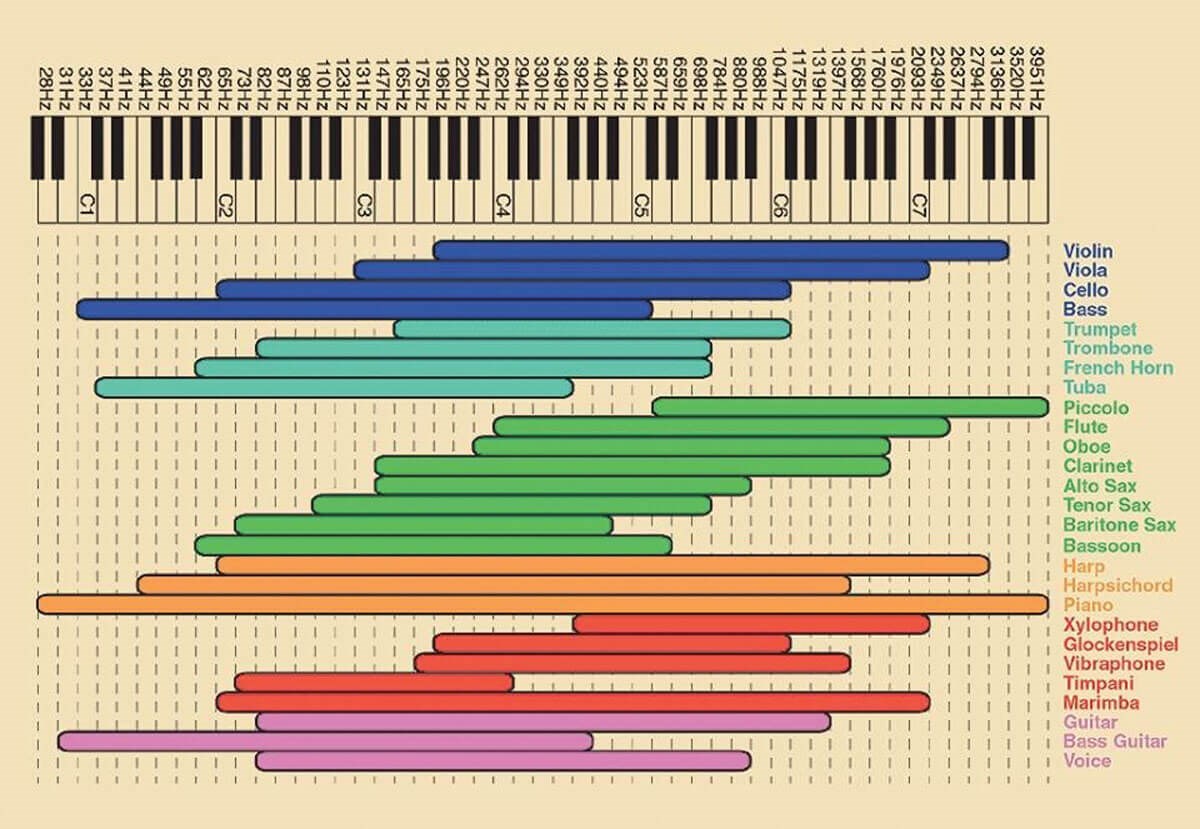
Figure 1. Chart for use in counselling, showing the frequency ranges of difference musical instruments.
Image by Alexyo.Netcom, CC BY-SA 3.0.
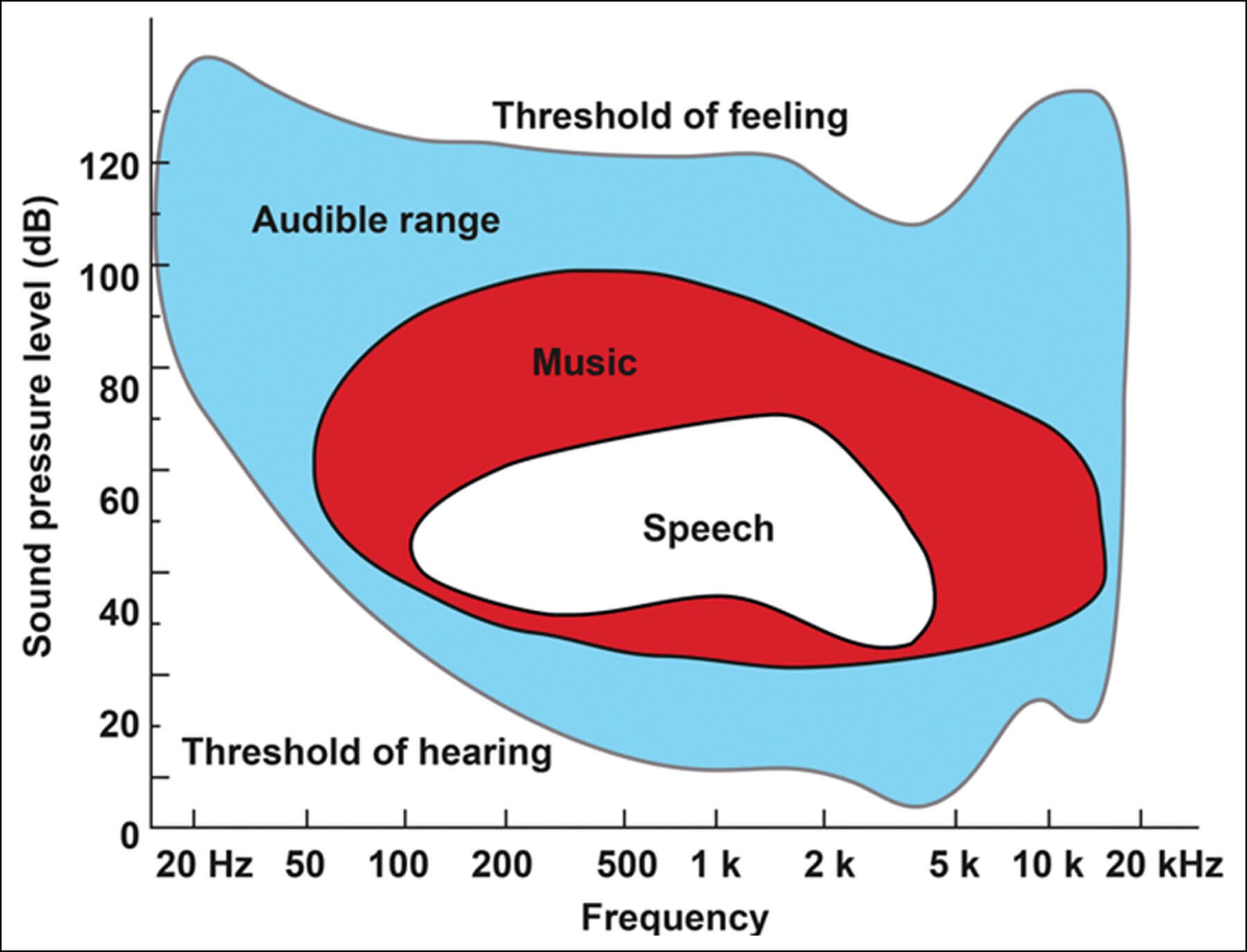
Figure 2. Music occupies extended frequency and dynamic ranges compared with spoken language.
Image from Ramirez T, Herbig R. Optimising hearing aid processing for music appreciation.
ENT & Audiology News 2016;25(4):101-2.
Specific fitting strategies
Audiologists in our study were asked to reflect on any fitting strategies they used to improve music listening, and responses were analysed thematically. Below we consider a few of the most frequently reported (see Greasley et al 2020 [1], p8 for a full list).
Disable automatic functions for speech. This included turning off feedback cancellation, noise reduction and microphone directionality. If a patient reports a problem with feedback, which is more likely in live music contexts, disabling the feedback manager prevents pure tone musical stimuli (e.g., organ, flute) being mistakenly analysed as feedback and suppressed. Similarly, with noise and wind noise management, disabling this functionality avoids musical stimuli being interpreted as unwanted sounds. There may be benefits to fixed microphone directionality for live settings, as audience and competing noise can be distracting. This can also allow focus on the music for performers, reducing loud input from behind so long as ambient noise (e.g., other performers) is audible.
RELATED TOPIC - Tap the box below
Alterations to compression were commonly cited, though answers were generalised (e.g., change compression type/settings, change compression ratios) which made it difficult to quantify specific adjustments. Studies have shown that slow-acting WDRC and linear amplification are associated with higher preference ratings for classical music than fast-acting WDRC [4] and that hearing aid users’ ability to pick out individual instruments was improved in the linear amplification condition compared to slow/fast-acting WDRC [5]. Though further research is needed, given evidence to date, we would advocate using slow-acting compression.
Changes to gain appeared frequently in responses, though some noted increased gain at high frequencies and others reported applying low- or mid- frequency gain, and there was a lack of specificity as to the degree of change or how these were applied across different frequencies or for differing input levels. Marchand explored the effects of changes in frequency-specific gain on preference for classical and jazz excerpts, finding that hearing-impaired listeners preferred gain with the maximum amount of low frequency emphasis [6]. Vaisberg et al found that hearing-impaired listeners preferred increased low-frequency gain compared to standard fitting formula for speech (DSLv5-adult), as well as decreased high-frequency gain for popular and classical music [7]. It seems there is a preference for increased low-frequency gain for music, however further research is needed.
“Open fittings reduce the build-up of self-generated low-frequency sound, which is especially beneficial for singers and performers”
Using the manufacturers music program. The use and efficacy of music programs is mixed. Madsen and Moore found some evidence that music programs made it easier to distinguish between individual instruments, but found no differences in aspects such as clarity and tone quality [2]. Looi et al found that those with a music program reported worse sound quality for music than their everyday program [8]. Overall, we would advise using a music program as this can be programmed to encompass other strategies. A trial will allow patients to assess benefit on a case-by-case basis.
Another reported strategy was adjusting Maximum Power Output (MPO) due to the higher dynamic range of music, though this needs to be done with care and within safe limits. Increasing MPO minimally allows more flexibility for adapting gain across frequency where WDRC is used and may enhance music clarity, though further research is needed to establish the beneficial effects of this. Another strategy was Use open fitting as this provides a more natural acoustic which the brain is used to interpreting, and listeners can use the natural acoustic cues for localisation. Open fittings reduce the build-up of self-generated low-frequency sound, which is especially beneficial for singers and performers.
Taking individual differences into account. Importantly, many audiologists emphasised that there is no ‘one-size-fits-all’ approach, and it is necessary to ask hearing aid users about the styles they listen to and about typical listening and performing contexts.
Developing evidence-based resources
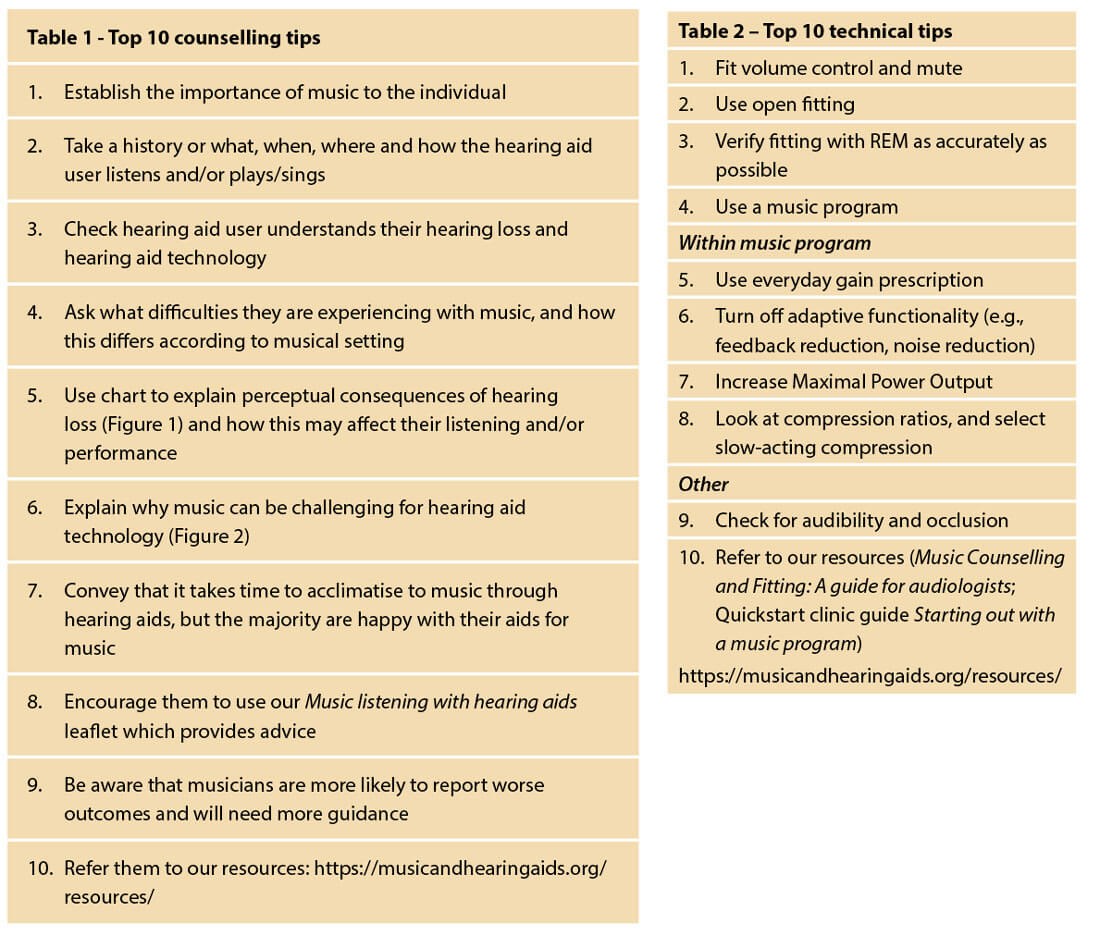
Our study is one of the first to map empirically the strategies that audiologists are using to address musical needs in clinic and, using the evidence, we have developed some counselling and technical tips for audiologists (see Tables 1 and 2). We have also developed resources for audiologists and hearing aid users that are freely available on our website. Due to the nature of the short survey, responses lacked specificity and there is a need for more in-depth research to consolidate these findings. Whilst the consistency with which audiologists reported these strategies means they are likely to be dependable, there is a need for systematic research relating clinical strategies to improvements in outcomes for music. This would provide an empirical evidence base for the development of validated guidelines to support training. The project team are currently on grant capture to continue research in this direction.
References
1. Greasley AE, Crook H, Fulford RJ. Music listening and hearing aids: perspectives from audiologists and their patients. International Journal of Audiology 2020;59(9):694-706.
2. Madsen SMK, Moore BCJ. Music and hearing aids. Trends in Hearing 2014;18: 2331216514558271.
3. Chasin M, Hockley NS. Special issue on music and hearing loss: Preventative and rehabilitative options. Trends in Amplification 2012;16(3):135‑82.
4. Croghan NBH, Arehart KH, Kates JM. Music Preferences With Hearing Aids: Effects of Signal Properties, Compression Settings, and Listener Characteristics. Ear & Hearing 2014;35(5):170-84.
5. Madsen SM, Stone MA, McKinney MF, et al. Effects of wide dynamic-range compression on the perceived clarity of individual musical instruments. Journal of Acoustical Society of America 2015;134(4):1867-76.
6. Marchand R. Hearing aids and music. Unpublished doctoral thesis, Macquarie University, Australia 2019.
7. Vaisberg JM, Beaulac S, Glista D, et al. Perceived sound quality dimensions influencing frequency-gain shaping preferences for hearing-aid amplified speech and music. Trends in Hearing 2021;25:2331216521989900.
8. Looi V, Rutledge K Prvan T. Music appreciation of adult hearing aid users and the impact of different levels of hearing loss. Ear & Hearing 2019;40(3):529‑44.
To download copies of our resources, go to www.musicandhearingaids,org/resources. We also have paper copies to distribute – if you would like copies, please get in touch with team on musicandhearingaids@leeds.ac.uk




