In the World Report on Hearing, launched by the World Health Organization (WHO) on 3 March 2021, the use of person-centred care is highly recommended. In this article, we learn about the history of person-centred healthcare and hearing care. But we start with the users’ voice, a foreword by Lidia Best, President of the European Federation of Hard of Hearing People.
The history of person-centred healthcare (PCC)
Most likely, the oldest known ethical code for healthcare practitioners is the Hippocratic Oath, of which the oldest found fragment dates to the year AD 275. But in this oath, you will not find any patient-centred reference. The first reference we found is the publication of Rogers in 1946, ‘Significant Aspects of Client-Centered Therapy’, in which he introduces the term “client-centred practice” in psychotherapy [1]. Another important step is the introduction of ‘goal attainment scaling (GAS)’ by Kiresuk and Sherman in 1968, where ‘goal setting’ with a patient, taking the patient’s lifestyle, preferences and aspirations into account, offers an opportunity for deriving a patient-generated outcome [2]. Nine years later, in 1977, Engel introduces the ‘biopsychosocial model’, where the healthcare provider works holistically and will focus on the whole person with a disease, as opposed to the traditional ‘biomedical model’ where the key focus is just the disease [3]. Only at the end of the 1980s is PCC gradually introduced by healthcare professionals.
The users’ voice: Lidia Best
I have used audiology and hearing care services for over 30 years. I had my share of good and bad experiences with hearing care professionals working in different countries and healthcare settings, though I was lucky to have support by audiologists already practising person-centred care (PCC).
PCC means practising real partnership: the patient and professional working together to make the best of what technology and wider society has to offer. It means that my hearing loss and functioning is seen in a much wider context of my lifestyle, my day-to-day activities, my aspirations, and goals. PCC means seeing a person, not a ‘walking audiogram’ and helping the person to understand their abilities and limitations, explaining the different available options. Through the partnership, we set out to make the best of the hearing technology available currently and, crucially, support personal choice. It is worth noting, informed choice and effective communication between healthcare professional and patient are central parts of the holistic approach; otherwise, we cannot claim to practise PCC.
PCC in ear and hearing care has the real potential to change lives in many ways. It is a win for the patients but also the professionals, thanks to improved satisfaction and overall results. Let’s make it happen!
The World Health Organization (WHO) is a strong advocate for PCC and defines it as follows: “Person-centred care addresses individuals’ health and social care needs rather than being driven by isolated health conditions or symptoms. A person-centred, integrated approach also embraces the context of individuals’ daily lives, including the impact of their health and needs on those close to them and in their communities.” [4] In 2013, the WHO European Regional office launched a report titled ‘Towards people-centred health systems: an innovative approach for better health outcomes’, where PCC is promoted as an approach that will lead to better outcomes and where it also states that healthcare is not always evidence-informed and rarely patient centred in Europe [5].
Does PCC lead to better health outcomes?
We evaluated nine systematic reviews with focus on the influence of PCC on health outcomes and these show careful positive conclusions, such as improved overall health outcomes, clinical effectiveness, healthcare utilisation, treatment adherence, and self-management or self-efficacy.
Is PCC the best approach for all patients?
Stewart states that “not every patient prefers a person-centred approach, and it may even be counter-productive or unwise. In fact, patient centred, means that you also individualise and take the patients preference for information and for shared decision making into account” [6]. But according to Turner and Archer, most patients are in favour of PCC [7]. They evaluated the patients’ perspective on PCC: 78% indicated that it’s important that the doctor is interested in their feelings and worries, 73% wanted to be included in the decision-making and 66% wanted the doctor to try and understand how they see things.
Is PCC implemented widely today?
In 2023, Havana et al conducted a systematic review on ‘Patients’ experiences of patient-centred care in hospital setting’ and they concluded that “the implementation and provision of PCC in hospitals is incomplete and patients’ involvement in their own care should be in the focus of PCC. The majority of patients experienced receiving PCC, but others did not” [8].
Is PCC accessible for everybody?
In 2023, Gahlon et al published a study in which they concluded that the odds of individuals with hearing loss having suboptimal perception of PCC was 17% greater compared to subjects with no hearing loss [9].
The history of person-centred hearing care (PCHC)
The first publication we found on person-centred hearing care (PCHC) was published in 1991, when Stephens and Hétu published ‘Impairment, disability and handicap in audiology: towards a consensus’, which is the introduction of the biopsychosocial model of care in audiology [10]. In 1997, Dillon et al introduced the Client Oriented Scale of Improvement (COSI – see Figure 1), a goal attainment scale (GAS) applied in hearing care [11]. According to English, this scale is a key element in PCHC and results in a treatment which addresses the problems of living with hearing loss, not the audiogram [12]. The IDA institute was founded in 2007 with the mission of building a community that embraces PCHC, and they did that by promoting PCHC during their training sessions and, later, in modules on their website.
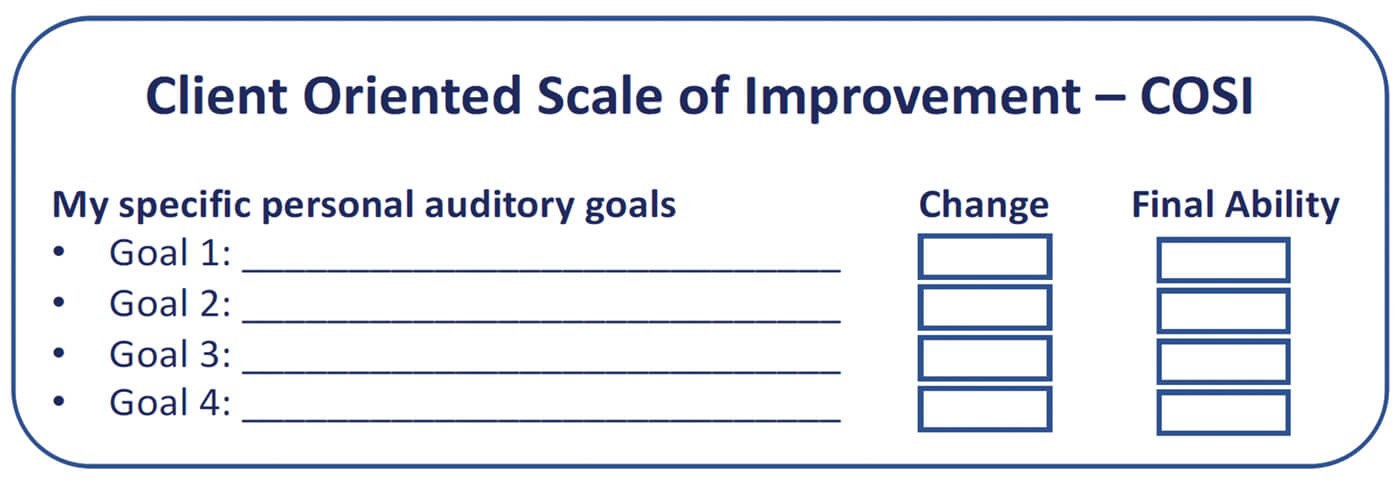
Figure 1.
Is PCHC implemented widely?
In contrast to PCC, which was rolled out gradually in the late 1980s, PCHC was introduced much later. Laplante-Lévesque et al mention that in 2010, “empirical data and publications on rehabilitative audiology decision making are hardly available” [13] and in 2014, Grenness concludes that “patient-centred care has received much less attention in audiology than it has in other areas of healthcare and more research is required to optimise patient-centred care in audiological rehabilitation” [14].
"Odds of individuals with hearing loss having suboptimal perception of PCC was 17% greater compared to subjects with no hearing loss"
In 2021, the WHO World Report on Hearing was published and has multiple sections and references to PCHC [15]. As with PCC, the World Health Organization is a strong advocate for PCHC. Hopefully, this will increase the interest and the number of studies on this topic.
PCHC needs to be an essential part of audiology education and practice, but more quality research and systematic reviews need to be conducted. Compared to PCC, we need to step up, in order to achieve better hearing health outcomes, clinical effectiveness, hearing care utilisation, treatment adherence, and self-management or self-efficacy.
References
1. Rogers CR. Significant aspects of client-centered therapy. Am Psychol 1946;1(10):415.
2. Kiresuk TJ, Sherman RE. Goal attainment scaling: A general method for evaluating comprehensive community mental health programs. Community Ment Health J 1968;4(6):443-3.
3. Engel GL. The need for a new medical model: a challenge for biomedicine. Science 1977;196(4286):129-36.
4. WHO. Integrated care for older people (ICOPE): guidance for person-centred assessment and pathways in primary care. 2019.
www.who.int/publications/i/
item/WHO-FWC-ALC-19.1
5. WHO. Towards people-centred health systems: An innovative approach for better health outcomes. 2013.
https://apps.who.int/iris/
handle/10665/372298
6. Stewart M. Towards a global definition of patient centred care: the patient should be the judge of patient centred care. BMJ 2001;322(7284):444-5.
7. Turner RE, Archer E. Patient-centred care: The patients’ perspective-A mixed-methods pilot study. Afr J Prim Health Care Fam Med 2020;12(1):2071-928.
8. Havana T, Kuha S, Laukka E, Kanste O. Patients’ experiences of patient-centred care in hospital setting: A systematic review of qualitative studies. Scand J Caring Sci 2023. Epub ahead of print.
9. Gahlon G, Oh ES, Reed NS. Association of perception of patient-centered care with hearing loss by race. J Am Geriatr Soc 2023. Epub ahead of print.
10. Stephens D, Hétu R. Impairment, disability and handicap in audiology: towards a consensus. Audiology 1991;30(4):185-200.
11. Dillon H, James A, Ginis J. Client Oriented Scale of Improvement (COSI) and its relationship to several other measures of benefit and satisfaction provided by hearing aids. J Am Acad Audiol 1997;8(1):27-43.
12. English K. Get ready for the Next Big Thing in audiologic counselling. The Hearing Journal 2005;58(7):10-5.
13. Laplante-Lévesque A, Hickson L, Worrall L. A qualitative study of shared decision making in rehabilitative audiology. J Acad Rehabil Audiol 2010;43:27-43.
14. Grenness C, Hickson L, Laplante-Lévesque A, Davidson B. Patient-centred care: A review for rehabilitative audiologists. Int J Audiol 2014;53(sup1):S60-7.
15. World Health Organisation. World Report on Hearing. 2021.
www.who.int/publications/i/
item/world-report-on-hearing
Further reading can be found in:
Laureyns M. PATIENT-, CLIENT-, PERSON- OR PEOPLE-CENTRED CARE General Health Care and Hearing Care – CRS Whitepaper 2022.
https://crs.amplifon.com/content/dam/
crssite/other-documents/it/publications/
2022-PCC-Health-and-Hearing-Care
-A-CRS-White-Paper.pdf
All links last accessed September 2023.
Declaration of competing interests:
Mark Laureyns is employed by the Amplifon Centre for Research and Studies in Milan, an international provider of hearing care, and by the audiology department of the Thomas More University College in Antwerp, an educational setting for audiologists.