How has clinical practice in the management of thyroid and parathyroid disease has evolved in recent years? I perform very few head & neck operations where the patient tells me just one week following surgery that they ‘feel much better’. A parathyroidectomy is one of them.
While traditionally falling within the domain of the general surgeon, data from the UK has shown that an increasing number of thyroid surgeries are now being performed by otolaryngologists [1]. Although there is no hard data yet, this is likely a worldwide trend. As otolaryngologists we should welcome this, but it is incumbent on us to familiarise and update ourselves and our trainees with the management of the various pathologies that occur in the thyroid.
Thyroid nodules are very common, and the majority are benign: they need no intervention other than observation. In the Western world, the number of thyroid cancers diagnoses have increased [2]. This is largely attributed to a jump in the detection of small papillary cancers due to frequent use of imaging procedures, often done for an unrelated reason. These ‘incidentalomas’ have led to an artificial epidemic of thyroid cancer. Most of these tumours would be clinically irrelevant if not detected incidentally, given the usually indolent biology and slow progression of the disease.

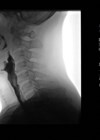
Thyroid and parathyroid surgery can be performed through very small aesthetic
incisions on the neck, making remote access/robotic approaches less appealing.
The classical treatment is the total thyroidectomy, but for small tumours there is an interest in developing alternative strategies for their management. ‘Active surveillance’, which is to keep a sub-centimetre papillary cancer under observation until signs of growth are evident, has been pioneered in Japan by a group led by Dr Miyauchi [3]. There is now an accepted role for treating low-risk papillary cancers with a hemithyroidectomy, which allows you to preserve half the thyroid gland and reduces the risk of recurrent laryngeal nerve injury and hypocalcaemia secondary to parathyroid gland injury.
“Remote access approaches using a robot or laparoscope inserted via incisions placed on the chest, axilla or retroauricular region are increasingly being explored”
Parathyroidectomies are usually performed for over-functioning parathyroid glands, in a condition called primary hyperparathyroidism. This disease is characterised by increased secretion of parathormone, which alters calcium homeostasis, with ensuing bone loss and other effects of elevated calcium levels in the blood. There are four parathyroid glands in the neck, but the development of an adenoma in a single gland is generally the cause of hyperparathyroidism. Traditionally, a bilateral neck exploration was done for this disease.
SEE ALSO
The operation involved making a large incision on the neck and tediously identifying and examining all the parathyroid glands, before removing the one found with the tumour. As normal parathyroid glands are quite small (smaller than a pea), and their location in the neck quite variable, a neck exploration could easily last for hours and still be unsuccessful in locating the offending gland. Today, we use imaging (ultrasound, sestamibi scan, 4D CT, and others) in order to preoperatively identify the abnormal gland. A small incision of about an inch can then be used to excise this gland in a more targeted surgical approach called a minimal access focused parathyroidectomy. It has a success rate comparable to the traditional approach, with the advantage of rapid recovery and only an overnight stay in the hospital.
“For an otolaryngologist with an interest in thyroid and parathyroid surgery these are exciting times”
Expertise in imaging is the backbone for a such an approach. In our institute, with a single person doing ultrasound over the past decade, this has now shown a superior diagnostic ability than the other tests [4]. However, the choice of imaging is institution-specific, as no test can locate the offending gland with absolute reliability. Assembling a team of dedicated members centred around an endocrinology team is a good way to initiate a parathyroid programme.
Preclinical hyperparathyroidism is increasingly being diagnosed, often following incidentally-detected increased calcium levels on blood work needed for other reasons. The use of multichannel AutoAnalysers since the 1970s for biochemical blood tests has contributed to this shift. In the developed world, this is the majority presentation and much of the focus is now on selecting patients who can be observed with published guidelines that are constantly updated [5]. In our part of the world, however, the overwhelming presentation is of symptomatic disease that affects the bones and kidneys. Much of the disease burden remains underdiagnosed and it is important to bring the awareness of primary care physicians to this possibility when a high calcium level is observed in any patient.
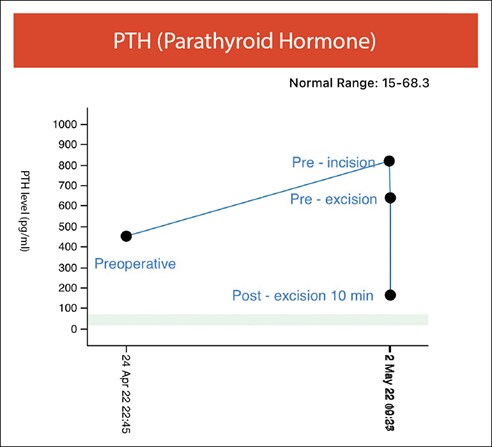
Focused parathyroidectomy must have intraoperative feedback mechanisms to ensure complete
removal of all hyperfunctioning parathyroid tissue. In this image there is adequate intraoperative
fall in PTH level after removing the enlarged parathyroid gland, indicating successful surgery.
Remote access approaches using a robot or laparoscope inserted via incisions placed on the chest, axilla or retroauricular region are increasingly being explored. While popular in the East Asia, particularly Korea, they are yet to find favour in large parts of the world. The advantage is primarily cosmetic, as the incision is placed in a less visible area, but its safety and efficacy is yet to be proven equivalent to the traditional approach. It is currently an option driven primarily by patient expectations, rather than a medical advancement, although time and further data would help clarify its eventual applicability.
“Preclinical hyperparathyroidism is increasingly being diagnosed, often following incidentally-detected increased calcium levels on blood work needed for other reasons”
For an otolaryngologist with an interest in thyroid and parathyroid surgery these are exciting times. Not only are we expanding into these fields but our repertoire of surgical approaches and technology is increasing as well.
References
1. Smith JA, Watkinson JC, Shaha A. Who should perform thyroid surgery? United Kingdom (UK) and United States (US) perspectives with recommendations. Eur Arch Otorhinolaryngol 2012;269:1-4.
2. Davies L, Welch HG. Increasing Incidence of Thyroid Cancer in the United States, 1973-2002. JAMA 2006;295(18):2164-7.
3. Ito Y, Miyauchi A, Kihara M, et al. Patient Age Is Significantly Related to the Progression of Papillary Microcarcinoma of the Thyroid Under Observation. Thyroid 2014;24(1):27-34.
4. Kaur P, Gattani R, Singhal A, et al. Impact of preoperative imaging on surgical approach for primary hyperparathyroidism. Data from single institution in India. Indian J Endocrinol Metab 2016;20(5):625-30.
5. Bilezikian JP, Brandi ML, Eastell R, et al. Guidelines for the Management of Asymptomatic Primary Hyperparathyroidism: Summary Statement from the Fourth International Workshop. J Clin Endocrinol Metab 2014;99(10):3561-9.